A Psych/ Medical Note template has been created for medical staff. The highlights of this note template are:
- Ability to push from certain sections of the previous “Psychiatric Note” template.
- Ability to retain previous note’s information so that authors can review what was written previously and push important medical information without having to retype.
- Pull real-time objective data such as vitals, allergies, labs and medications/orders.
- Keyphrase functionality can be leveraged to create custom text template within the textbox.
- Flexibly select relevant sections pertinent to the visit and document efficiently via customized text templates by individual or clinic/unit.
- Allow for documentation of medication consent.
Please click here for Instructional Video
How to Get to the Psych/Medical Note
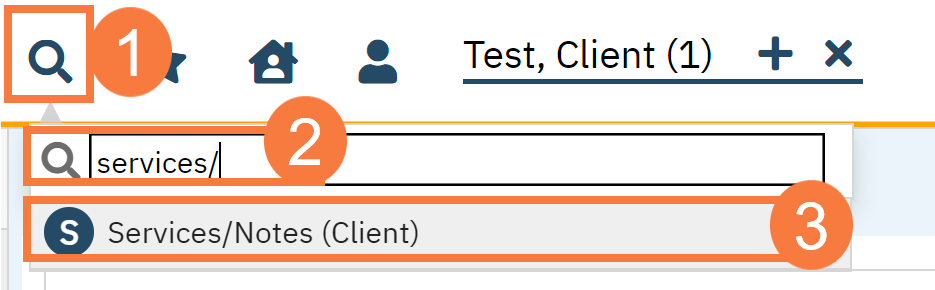
- With an active client selected, click the Search icon.
- Type Services/ into the search bar.
- Click to select Services/Notes (Client). The Service Note screen opens.
- Click the New icon.
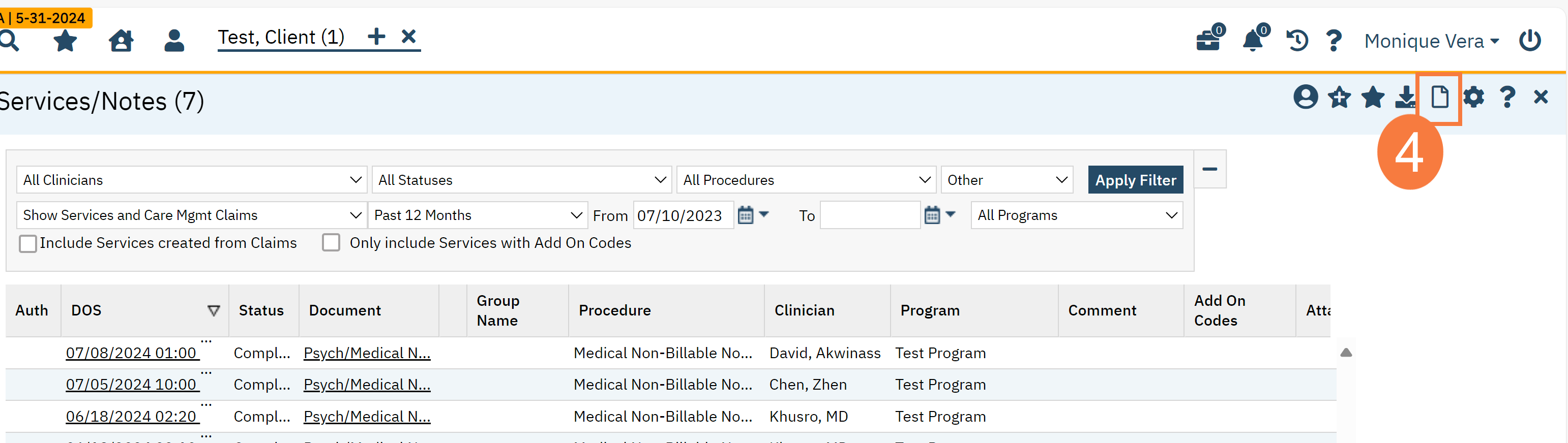
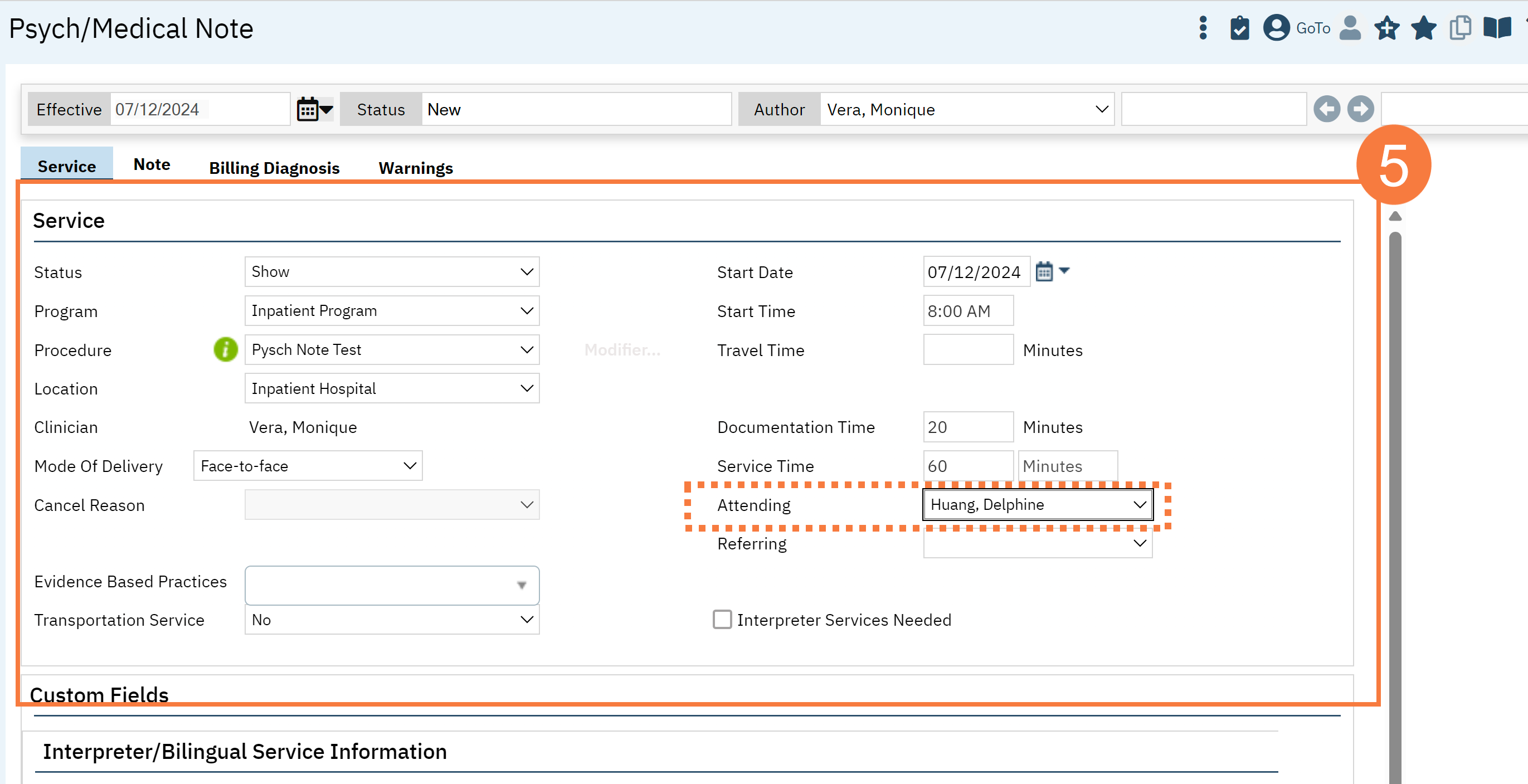
- This will take you to the Service Note screen. Complete the Services tab.
Note: fields with an asterisk * will show up on your final PDF.
- Status*
- Program*
- Procedure*
- Location*
- Mode of Delivery
- StartDate*
- Start Time*
- Travel Time (if needed)
- Documentation Time
- Service Time*
- Attending (if needed)*
Note: The same requirements will apply for marking Status, Program, Procedure, Location, Mode of Delivery, Start Date, Start Time, and Face to Face Time as all other billable service notes.
A new feature is allowing for a supervisor’s name to be selected as “Attending,” and this will show on the final pdf. If there needs to be other co-signers, then please follow instructions to assign co-signers. CLICK HERE for the article.
Please click here for Instructional Video
- Click the Note Tab.
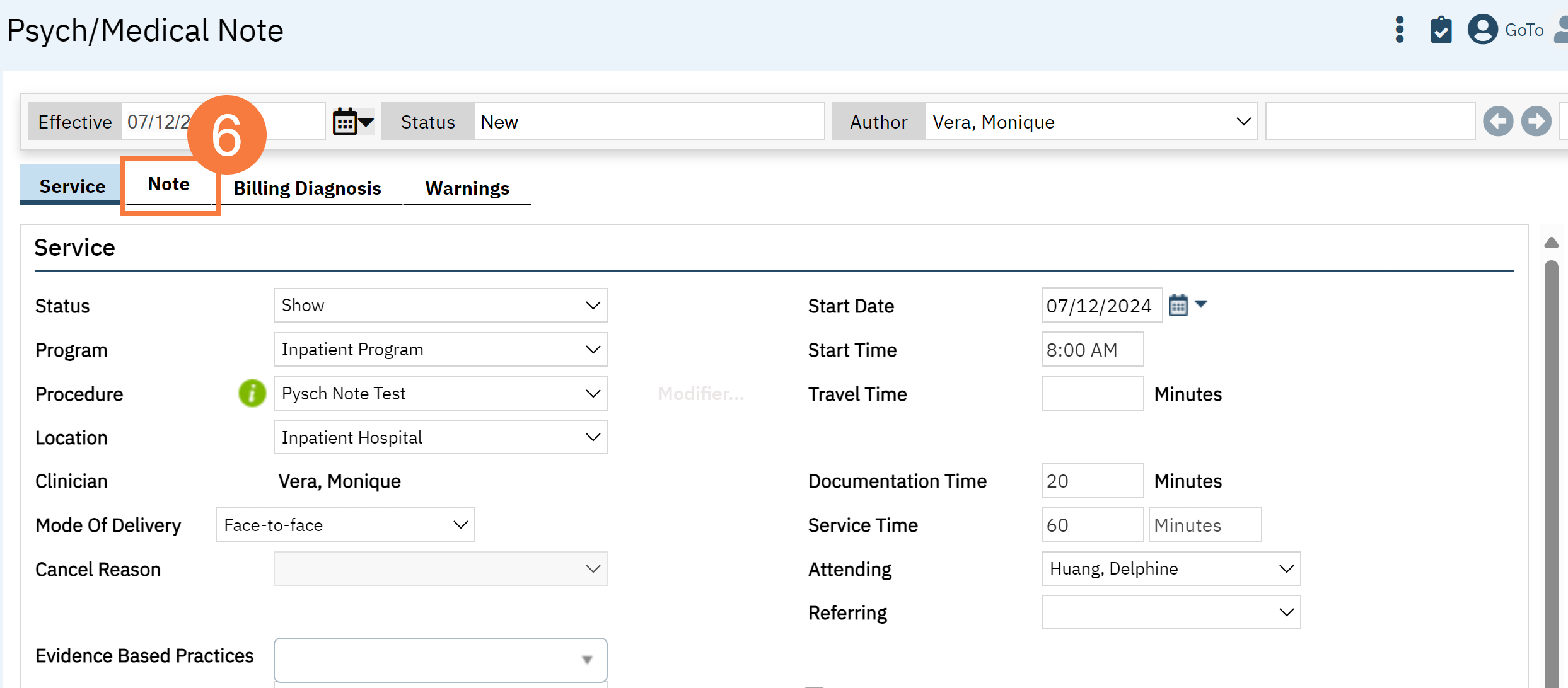
General Note Template Functionality
To see what procedure codes are defaulted to be associated to the new Psych/Medical Note template CLICK HERE. You will need to be permissioned and licensed to use these procedure codes.
Please click here for Instructional Video
Required fields:
- There are no required fields in the psych medical note template. This was intentional to give end users the flexibility to choose which textboxes to utilize.
How data from this template is stored and pushed to subsequent notes:
- For counties that are moving from old Psychiatric Note template to the new Psych/Medical Note, please CLICK HERE for information.
- With this new template, every textbox section will pull the most recent data that has been saved (even in draft form) or signed as a final PDF. It will push that information to the subsequent note as long as it is the same client and same author. . This means that initialization can occur across programs. If this is not intended, then user will need to manually remove data.
- Subsequent notes will initialize the textbox field data if you click “Save” or “Sign” and did NOT have a checkbox mark for “Delete from the Note.” It will indicate when this data was last updated in case you need to reference back to a previous “Sign” and did NOT have a checkbox mark for “Do not include in PDF/Delete from the Note.” It will indicate when this data was last updated in case you need to reference back to a particular note.
- If a different procedure code is used and the Psych/Medical Note template is used for those codes, the information will still carry over.
- Objective data/tables will follow CDAG rules, except where CDAG does not apply within SmartCare already (e.g. medications, allergies)

"Delete from Note" Functionality
This functionality was created to allow you to select only the sections relevant to the note and maintain a preview of information that may be historically important. This is done with the goal to avoid “chart bloat.”
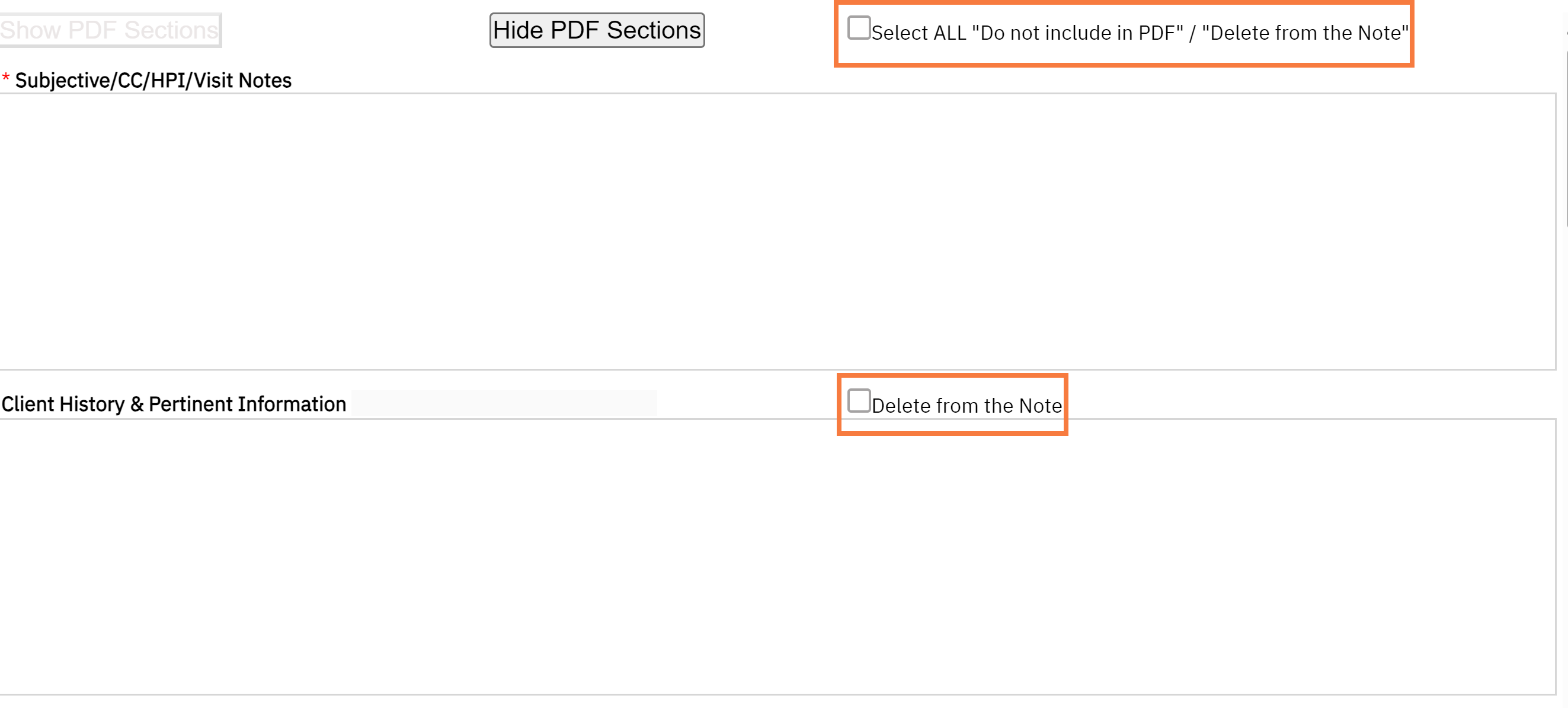
If “Delete from the Note” is selected for specific section, then that data will not show up on the signed PDF. If you would like to preview the note, click on “Hide PDF Sections.” If you would like to view all sections, then click “Show PDF Sections.” There is a checkbox called “Select ALL Do Not Include in PDF/Delete from the Note” which will allow removal of all sections except for the required sections “Subjective/CC/HPI/Notes” and “Assessment and Plan.”
If “Delete from the Note” is selected, then the textbox sections will NOT save once signed. If saving is desired, then you MUST REMEMBER to remove the checkmark. Checkmarks will be retained for subsequent notes.

Refresh of Data and Tables
While we recommend saving drafts often, the objective data will refresh every time you go to a different SmartCare screen. For example, if you go to enter a new Diagnosis Document, then this information will push into the note, when you return to screen even if the note has not yet been saved.
If for some reason the data from external tables is not refreshing, then you can manually refresh your page by clicking the “Refresh” button.
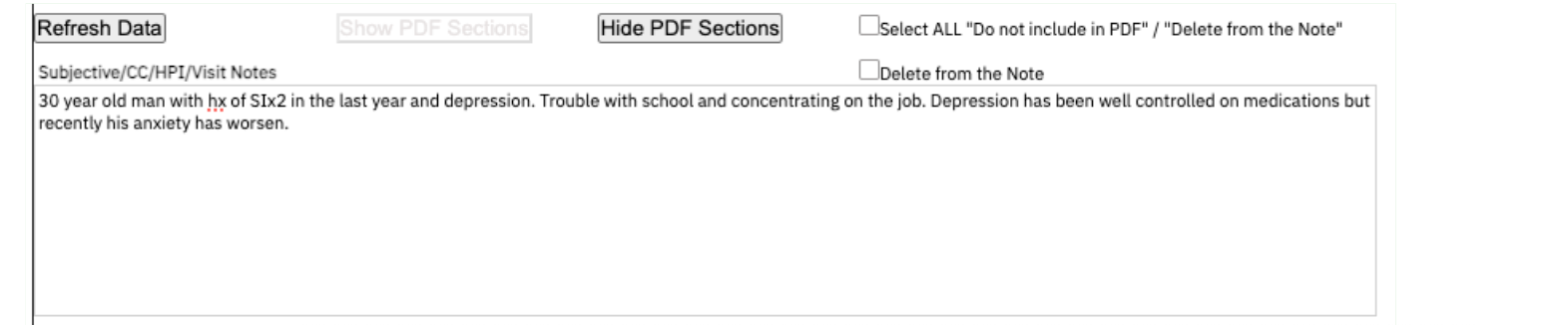
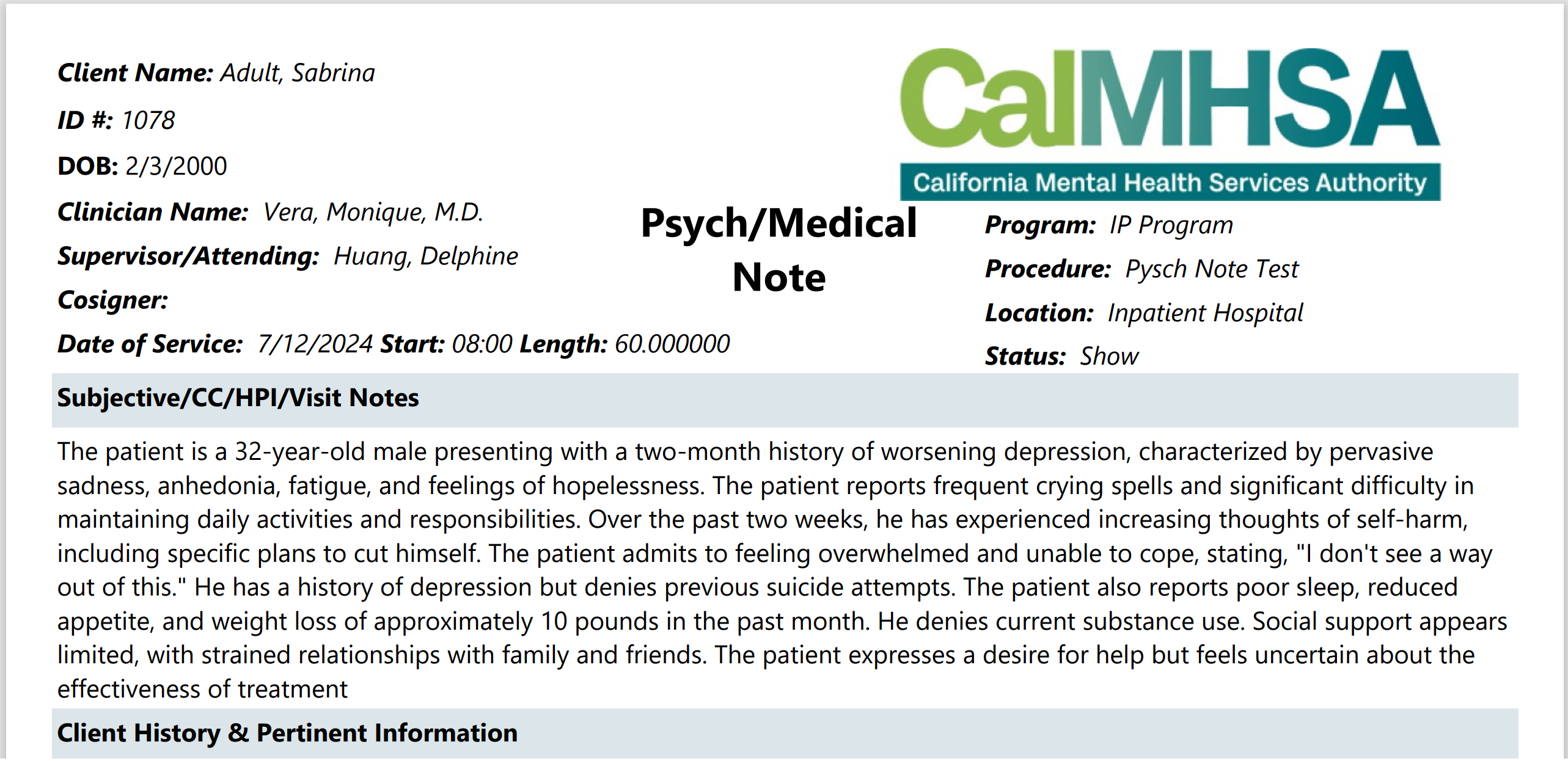
Subjective/CC/HPI/Notes Section
This section can be used to capture the subjective part of a patient visit. It can also be used to record chief complaints and if you choose not to document using any other sections, you can store the history of present illness and/or other notes here. The “Delete from Note” functionality can be utilized.
Client History and Pertinent Information
This section can be used to capture the patient’s history such as their previous psychiatric, medical, medication, or program history. It can also be used to capture any social, substance use, family history, pertinent tests. The “Delete from Note” functionality can be utilized.

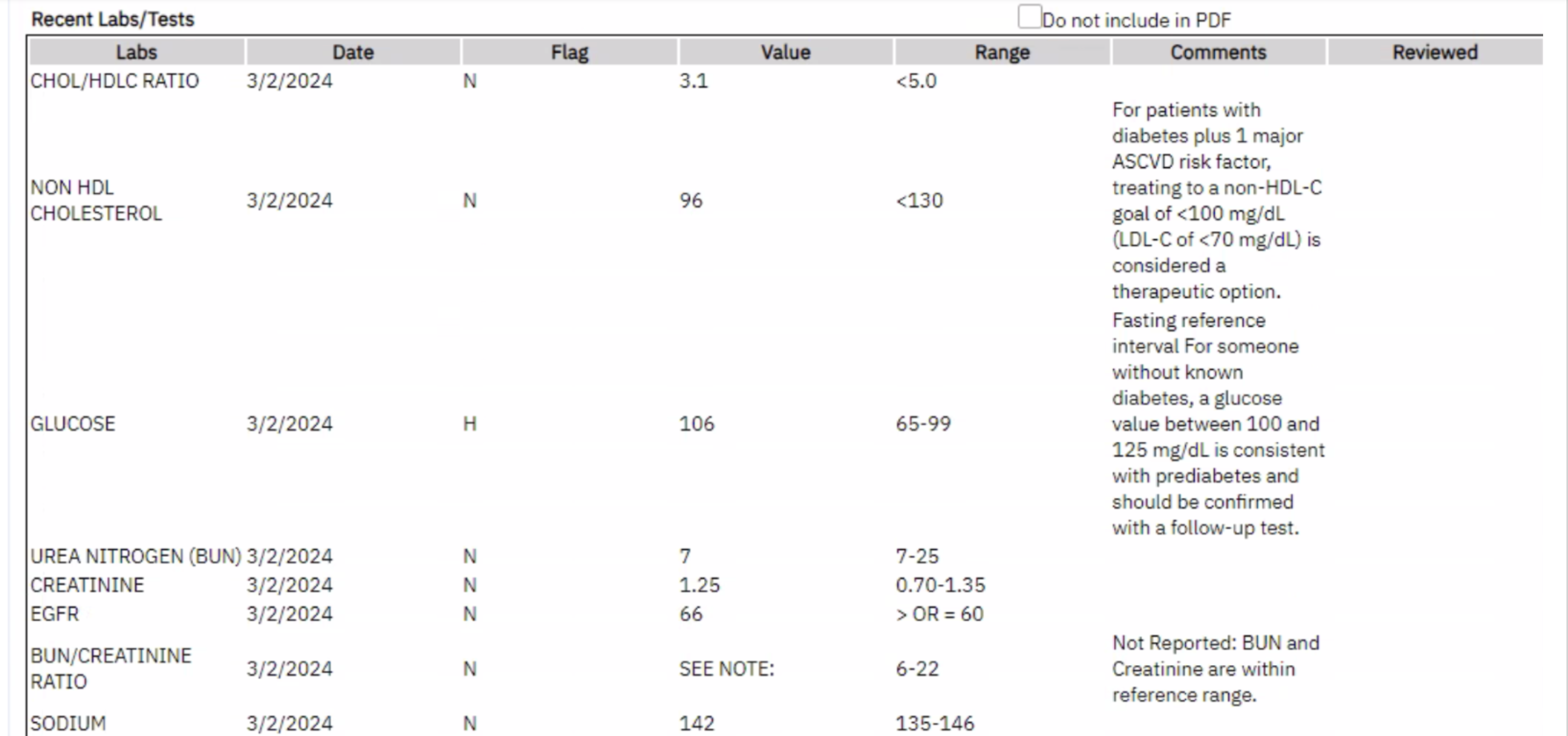
Recent Labs/Tests
This section pushes two months of lab data into the note. It includes the lab name, collected date, if any abnormality (H = high, L= low, N=Normal), the lab value, the range, lab comments, and if it has been reviewed by staff. The “Do Not Include in PDF” functionality can be utilized. If you wish to view comprehensive labs trends, then we recommend using the Comprehensive Lab Flowsheet Report. Each cell has a character count which if over that limit will show “…” You can hover over to read the additional text in the draft mode. However, the final PDF will only display up to the character count. The “Do Not Include in PDF” functionality can be utilized.
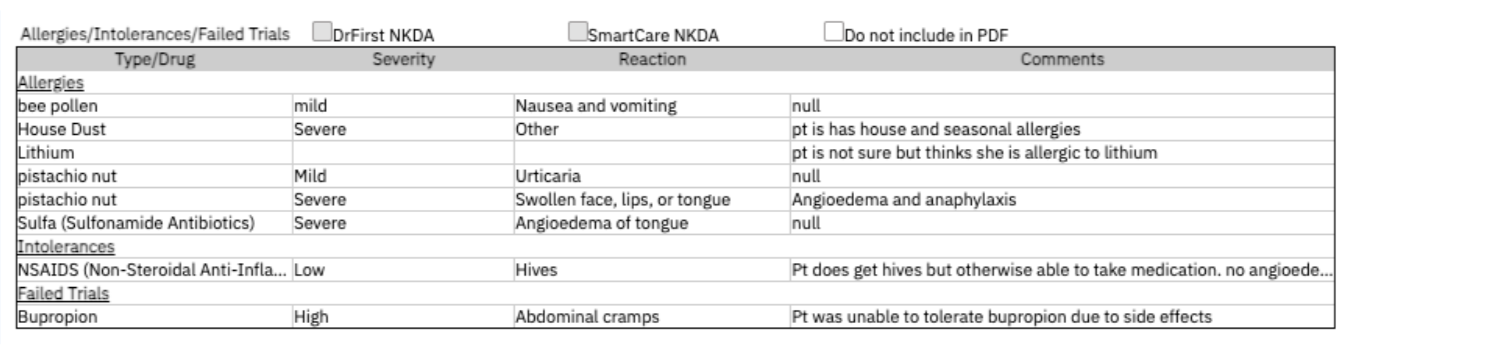
Allergies/Intolerances/Failed Trials
Allergies from CalMHSA Rx and SmartCare will be pushed into your Psych Medical Note template under the category “Allergies.” Please note that there can be up to a 5-minute delay or you can use the manual “Refresh” button to get updated tables. For SmartCare, each allergen will be categorized into Allergies, Intolerance and Failed Trials for CalMHSA Rx, allergens will all be listed under Allergy category. It will list the severity, reactions and comments (available only for SmartCare). Each cell has a character count which if over that limit will show “…”. You can hover over to read the additional text in the draft mode. However, the final PDF will only display up to the character count.
If a patient has not yet had their allergies reviewed within the e-prescribing system, then the NKDA checkbox will be not marked and grayed out. If NKDA/NKA has been marked, then the box will gray out depending on the source.

Note: If the same allergen (or NKDA/NKA) has been listed in multiple systems, then these will be listed as duplicates in this report, and there is no mechanism to capture any discrepancies.
The Do Not Include in PDF” functionality can be utilized.
The Refresh button can be used to manually push data if those updates are not appearing in your draft.
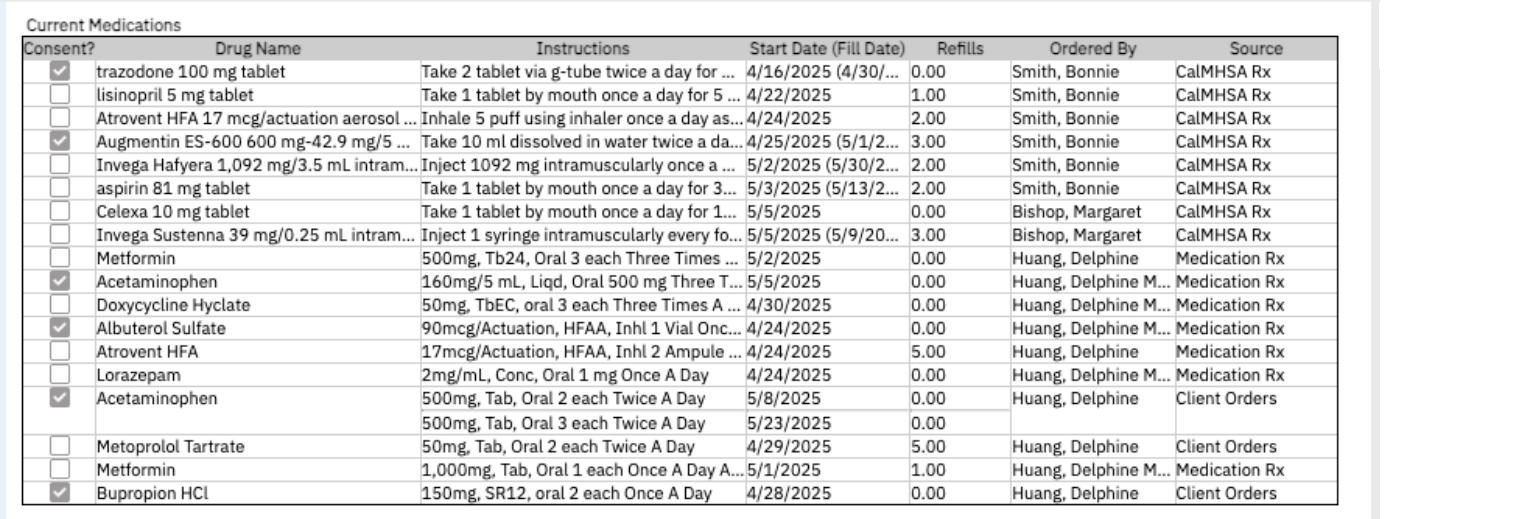
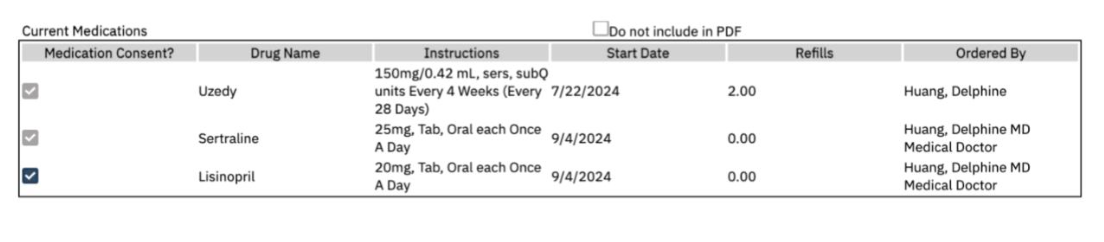
Current Medications
This section will pull medications from CalMHSA Rx and/or SmartCare’s Client Orders and Medication Rx. It will only display medications that are active and the end date has not expired within 1 year. It will include the start date (fill date), the number of refills and who prescribed the medications. It also will display the e-prescribing system under “Source” column.
Each cell has a character count which if over that limit will show “…”. You can hover over to read the additional text in the draft mode. However, the final PDF will only display up to the character count.
Please note that if the same medication has been listed in multiple systems, then these will be listed as duplicates in this report, and there is no mechanism to consolidate or capture any discrepancies. In addition, complex orders, such as titrations, may be split across multiple rows and display current or future steps, due to technical issues.
The “Do Not Include in PDF” functionality can be utilized.
The Refresh button can be used to manually push data if those updates are not appearing in your draft.
Note Regarding Medication Consent:
In most situations, a separate, signed “Medication Consent” document is no longer required. Consents for medications can be captured/documented in the prescriber’s progress note. These recommendations are specific to consents for medications and not general informed consent/consent to treat.
To review the CalMHSA protocol and memo by Manatt, CLICK HERE. You can also find the vetted templates and suggested use cases.
To use CalMHSA’s medication consent template, CLICK HERE for more information.
To learn more about Medication Consent Keyphrases, CLICK HERE.
If verbal or written consent is captured for certain medications (for example: antipsychotics, controlled substances, you can checkbox next to the medication name. This will generate a document automatically when the checkmark is placed. (whenever the document has been “Save” or “Signed”). This will save in Documents (Client) titled “Medication Consent – [Drug Name].
To learn more about a client–specific report of medication consents from services notes using the Psych Medical Note template, CLICK HERE.
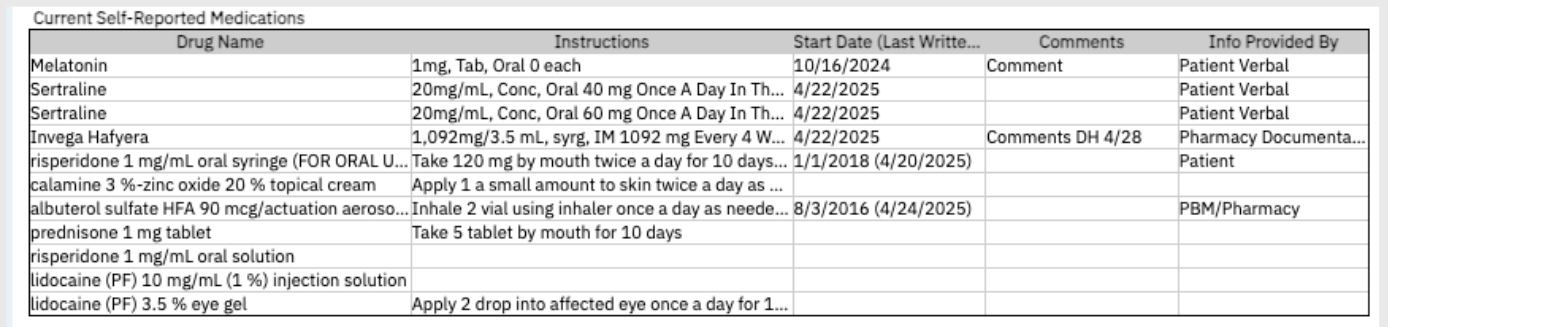
Current Self-Reported Medications
This section will push medication from CalMHSA Rx and from SmartCare Rx that are listed as part of a client’s medication list but are not prescribed within the platform. It will only display medications that are active, and the end date has not expired. It will include “Comments” (for CalMHSA Rx, this data is coming from “Office Use Only” field and “Source”. The Start Date is displayed here (along with the Last Written Date, if available for CalMHSA Rx only).
Note: If the same medication has been listed in multiple systems, then these will be listed as duplicates in this report, and there is no mechanism to consolidate or capture any discrepancies. In addition, complex orders, such as titrations, may be split across multiple rows and display current or future steps, due to technical issues.
The “Do Not Include in PDF” functionality can be utilized.
The Refresh button can be used to manually push data if those updates are not appearing in your draft.
Current Orders- Non Medications
This section will push active orders that have not yet expired, that are non-medications (e.g. Nursing, Additional, Labs etc. from Client Orders. It will include the Type of order, the order name/description, the start date and who ordered it.
The “Do Not Include in PDF” functionality can be utilized.
The Refresh button can be used to manually push data if those updates are not appearing in your draft.

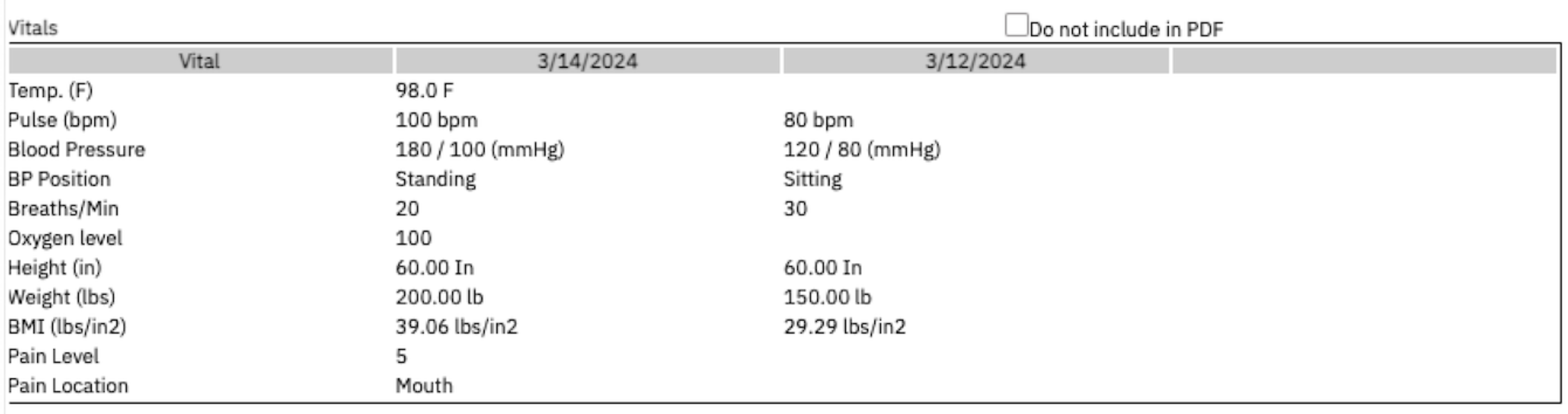
Vitals
This section will pull the last 3 vitals within a CDAG from the “Vitals/Meaningful Use” Flowsheet or “Enter Vitals”. This information will refresh the note automatically with any added information. The “Do Not Include in PDF” functionality can be utilized.
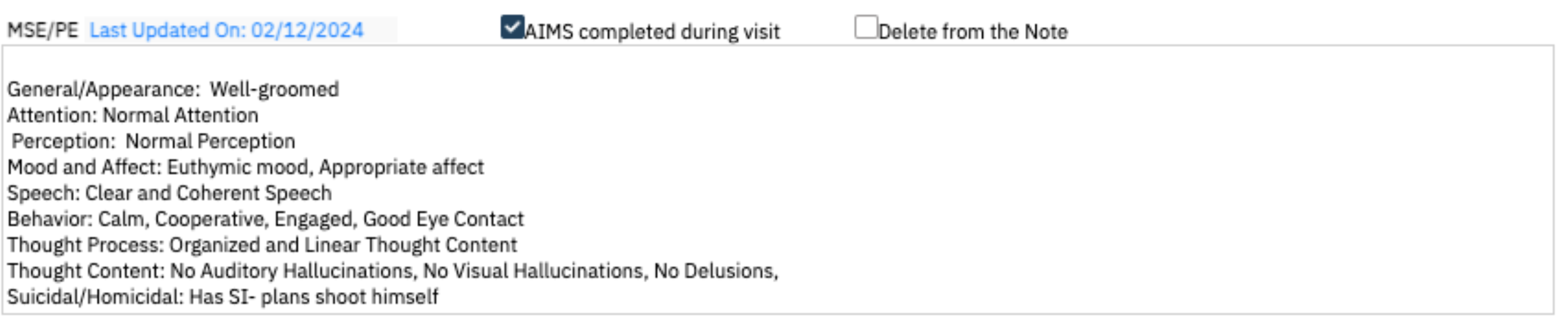
MSE/PE
This is a section that can be used to document the Mental Status Exam or Physical Exam. Key Phrases can be customized to create MSE templates to improve efficiency. The “Do Not Include in PDF” functionality can be utilized.
AIMS Completed During Visit
- There is also a checkbox to indicate if AIMS has been completed and the date will be displayed on the Client Medical Facesheet as a way to help other users know when it was last completed. The actual data collection should be completed in the AIMS Assessment Document. This checkmark will NOT be retained for the subsequent note.
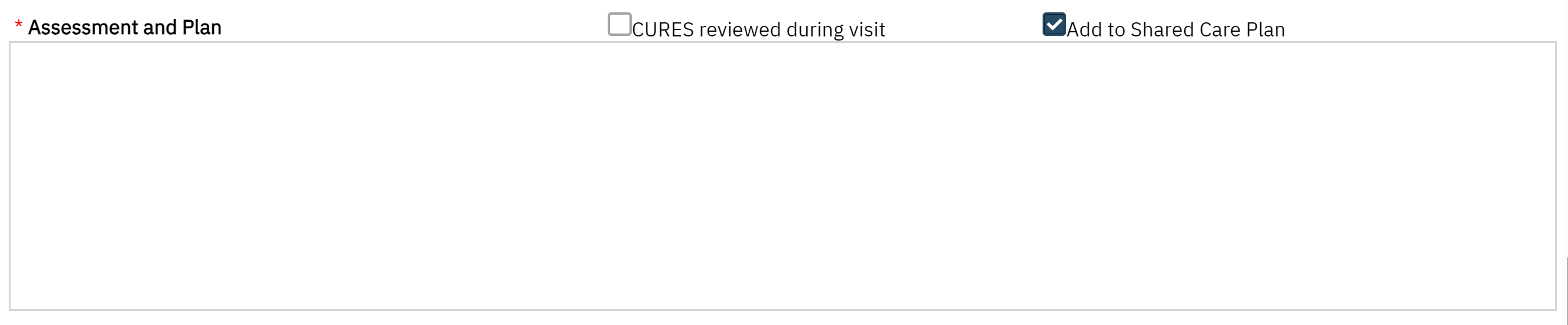
Assessment & Plan
Documentation of CURES: If CURES is being reviewed this can be check marked. This information will be displayed on the Client Medical Facesheet as an efficient way to see when it was last completed and by whom. This checkmark will NOT be retained for the subsequent note.
Add to Shared Care Plan: This is optional as we are still building out a future-state Shared Care Plan to be more collaborative and efficient in data collecting and data sharing. The goal is that for facilities that use a shared care plan or treatment plan, individual’s plans can feed into the document to reduce the need for double entry. For now, if the box is checked, this saves to the Shared Care Plan Report which is a compilation of individual’s psych medical note’s plans. This checkmark will NOT be retained for the subsequent note. CLICK HERE for more information.
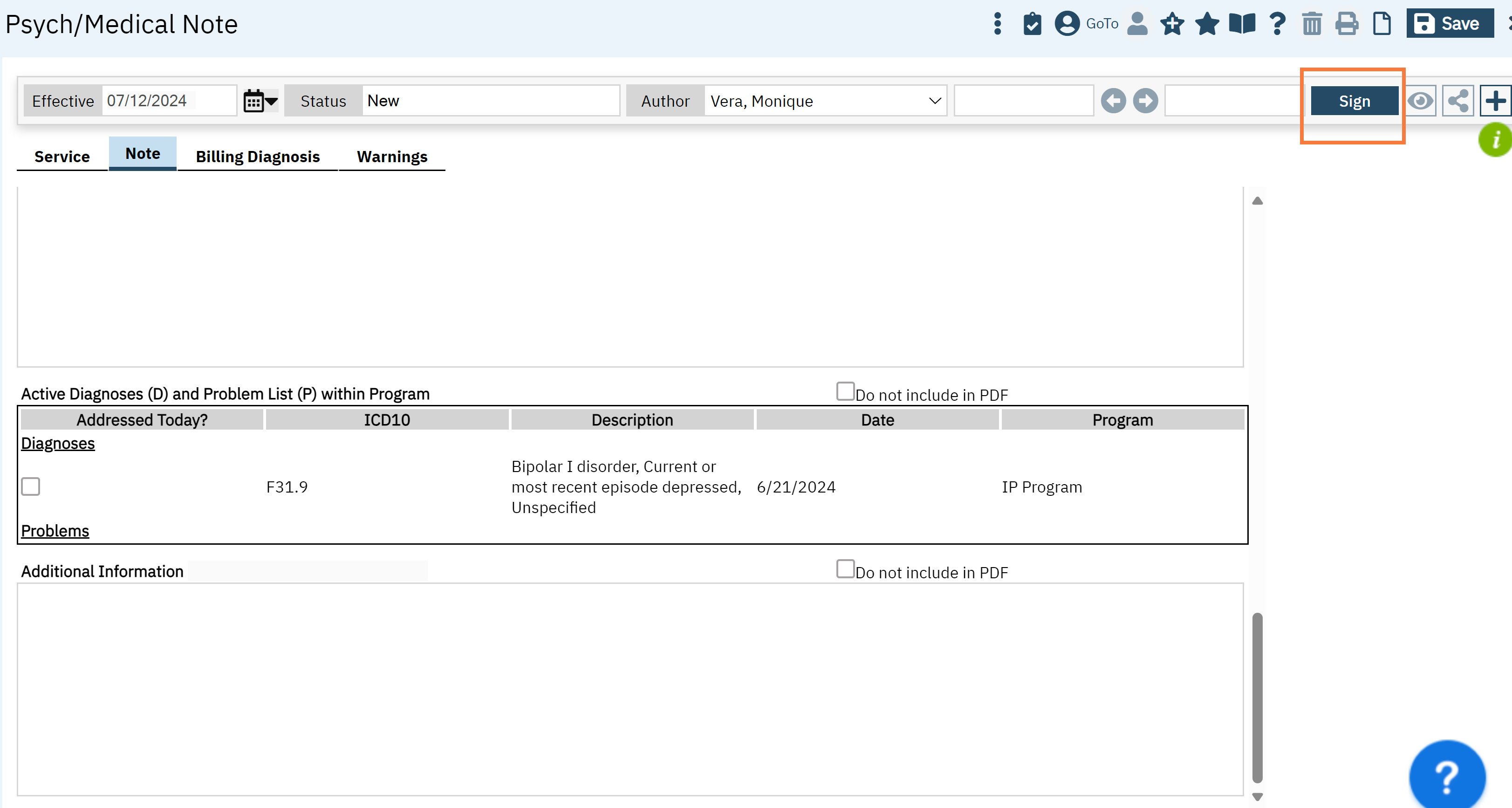
Active Diagnoses and Problem List within Programs
This section captures the client’s diagnoses and problem list from any programs that are within the same CDAG. The active diagnosis captured by Diagnosis Document is included in the diagnosis sub-section. Also, any problems that are documented in the Client Problem List are demarcated in the second subsection. Any common ICD10s are grouped together. The date represents the most recent entry for that ICD10 code. You can checkmark the issues that were addressed at the visit. Any selection will NOT retain its checkmark for the subsequent note. The “Do not include in PDF” functionality can be utilized.

Additional Information
This section is a flexible section for authors to capture information that does not fit in any above section but should be included. (For example: attestation, client’s timeline within the program, family conversations, follow-up information). The “Do Not Include in PDF” functionality can be utilized.
Complete Note
To complete a note, the author must sign the note by clicking the “Sign” blue button on the upper right corner. The proxy and cosign workflow remains unchanged. Your document will generate.
- Last Updated:May 14, 2025