The purpose of this report is to compile relevant client specific medical information that is commonly used upon discharging a patient from a program, transfer to another provider/clinic/unit. It can also be used to provide an aftercare summary with medical-related information for the client and/or family.
This report is medically focused because it allows for selection of medications, orders, and labs. It is used in conjunction with CalMHSA Discharge or Transfer Summary which allows for written text.
NOTE: SmartCare’s Summary of Care, Discharge Summary, and CalMHSA’s Discharge Instructions can also be used for discharge documentation but are not linked to this particular report.
In addition, if your facility is required by to create a Care Coordination Plan, as part of the BHIN –24-039, for discharging individuals experiencing temporary holds or conservatorship, then this report can support many of the data fields required by the plan. For more information, click here.
The defaulted users that have access to this are those with permission to Medication Rx, Add Medications Prescribed Elsewhere, Add Pharmacies to Rx, Prescriber, IP/CSU/Res, Medical IP/CSU/Res, CalMHSA SysAdmin, Allergies and Flowsheets, and Medical Supervisor.
A client must be selected in order to run this report.
- With a client open, click the Search icon.
- Type Aftercare in the search bar.
- Click to select CalMHSA 119 Aftercare/Discharge/Transfer Summaries Report (Client).
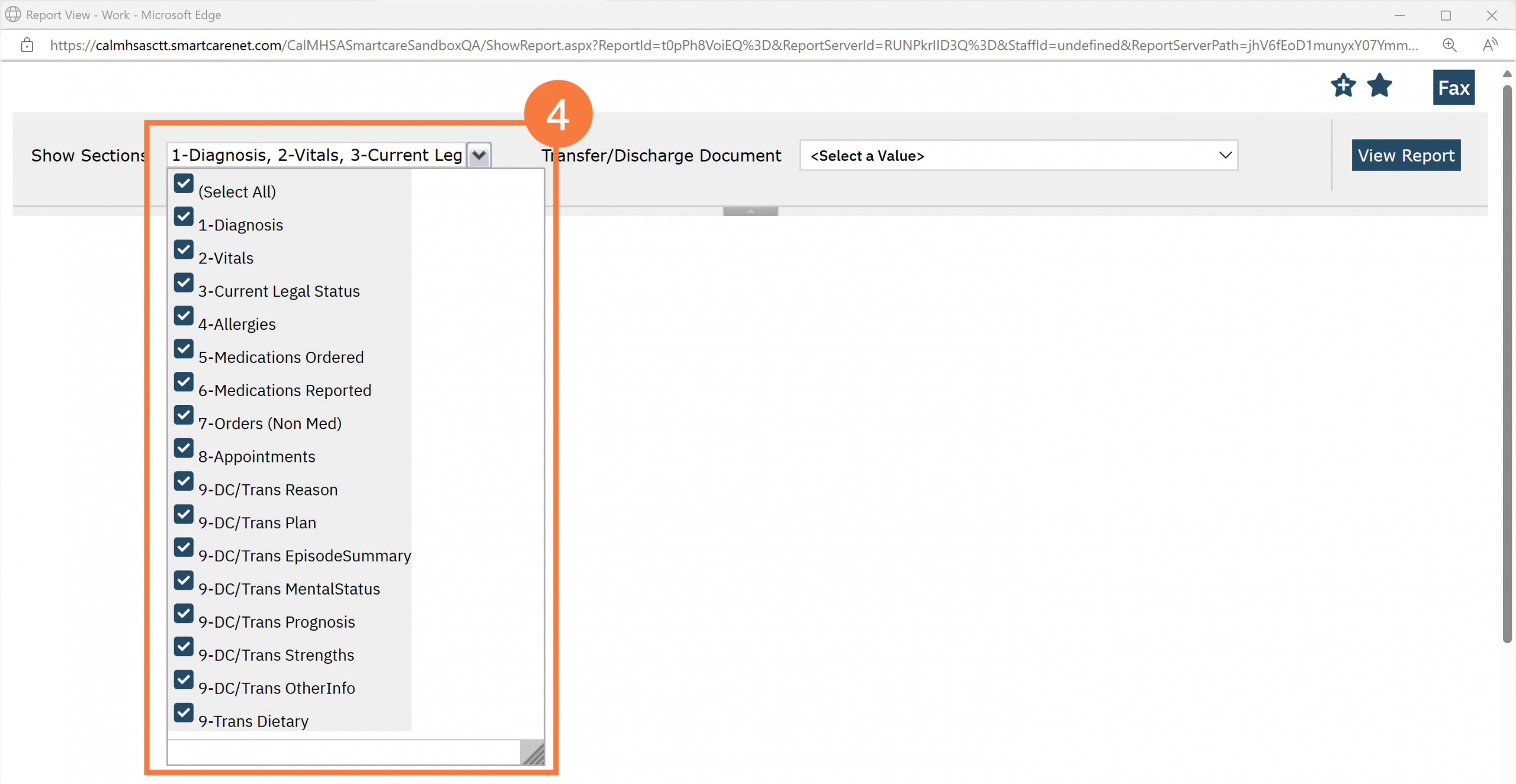
- The report view window will open. Click the Show Sections menu drop-down and unselect the fields you don’t want on the report. Leave all selected to view all fields on the report.
- Note: For the field options labeled as 8– DC/Trans [Section Title] these refer to the textboxes of the document “CalMHSA Discharge Summary” or “CalMHSA Transfer Summary”. Those documents are editable and you can write you can write any specifics. Those textboxes are what populate into their respective sections in this report.
- Note: Use the arrows in the report to advance pages.
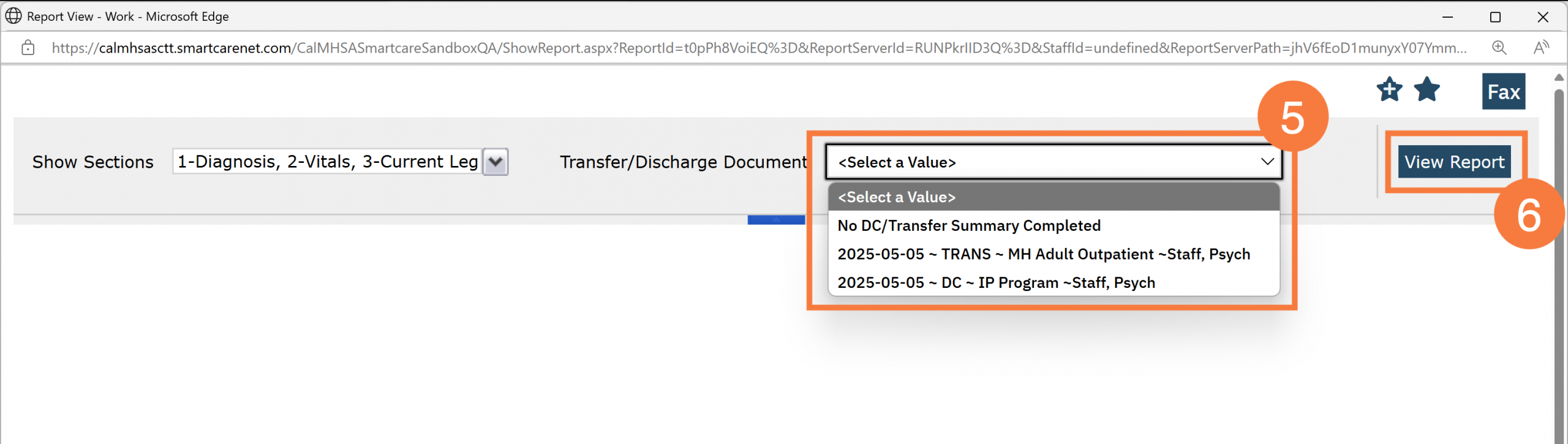
- In the Discharge Document field, click the drop-down menu and select the relevant CalMHSA Discharge or Transfer Summary from the list by Effective Date, Program and Author. Only one summary can be selected at a time. You will only see the options within your CDAG.
- Note: You can also select “no discharge summary was completed.” If that is the case, then the “Discharge/Referring Facility”, “Transfer Point of Contact”, and “Discharge/Transfer Plan” sections of the output will be suppressed.
- Click View Report.
Client Information & Discharge/Referring Facility
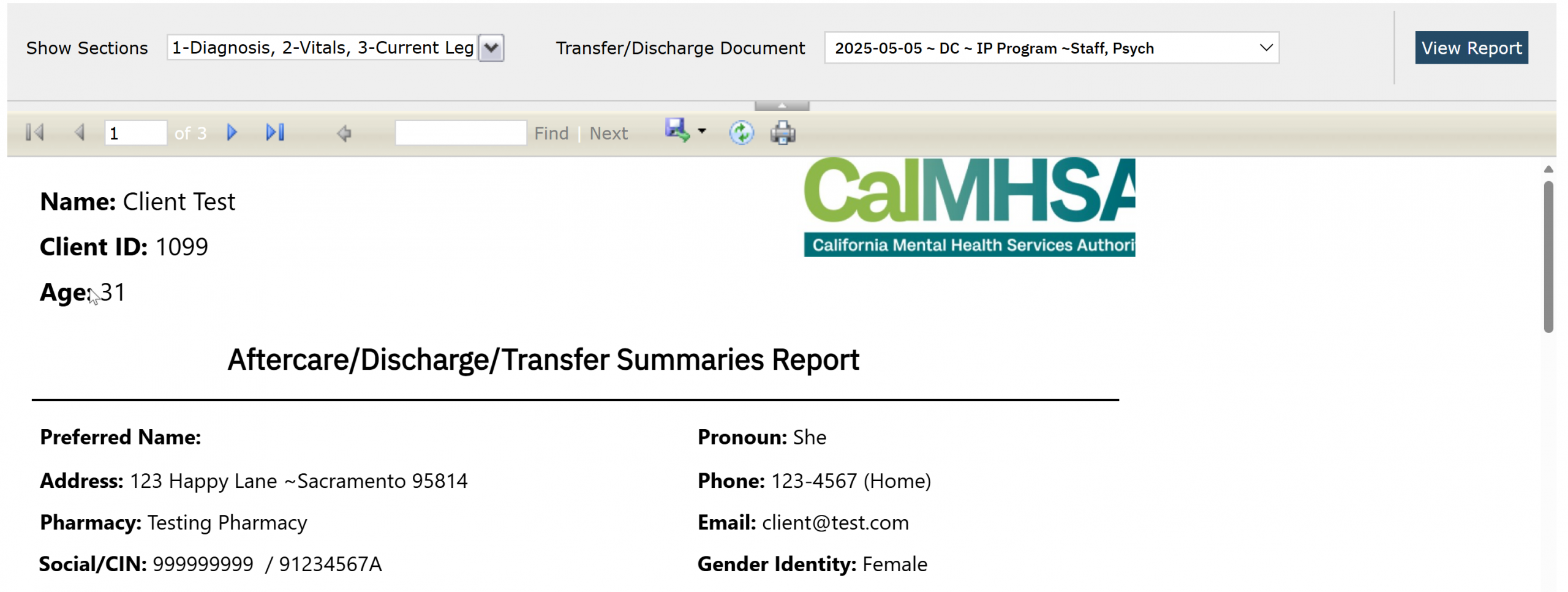
- All reports will include the patient name, client ID, and age.
- It will also include the following if there is data present in these fields; the chosen name (if under “Alias”), pronouns, address, phone, email, and preferred pharmacy (only displayed for SmartCare’s Medication Rx Module).
Discharge/Referring Facility
This section is based on the CalMHSA Discharge or Transfer Summary document that was selected above.
- If the CalMHSA Discharge Summary is selected then you will see the author of that document is presumed to be the discharging provider. The “Discharging Practitioner” field will be blank. It will also list the program associated to the CalMHSA Discharge Summary document and the program address, program location, program phone number, admit date, discharge date, and effective date of the document.
- If the CalMHSA Transfer Summary is selected: The author of that document will be listed under “Author of DIscharge/Transfer Summary” and if there was a Discharging Practitioner selected, then this will be listed. It will list the program associated to the CalMHSA Transfer Summary document and list the program address, program location, program phone number, admit date, discharge date, and effective date of the document.
- If No DC/Transfer Summary Completed is selected as the parameter, then this section will not appear.
Transfer Point of Contact
If the selected CalMHSA Transfer Summary document has this information, the data will initialize into this section.

Diagnosis and Problems
If this information is available in either Diagnosis Document and/or Client Clinical Problems for the specified program related to the selected CalMHSA Discharge or Transfer Summary, then this data will initialize into this section.
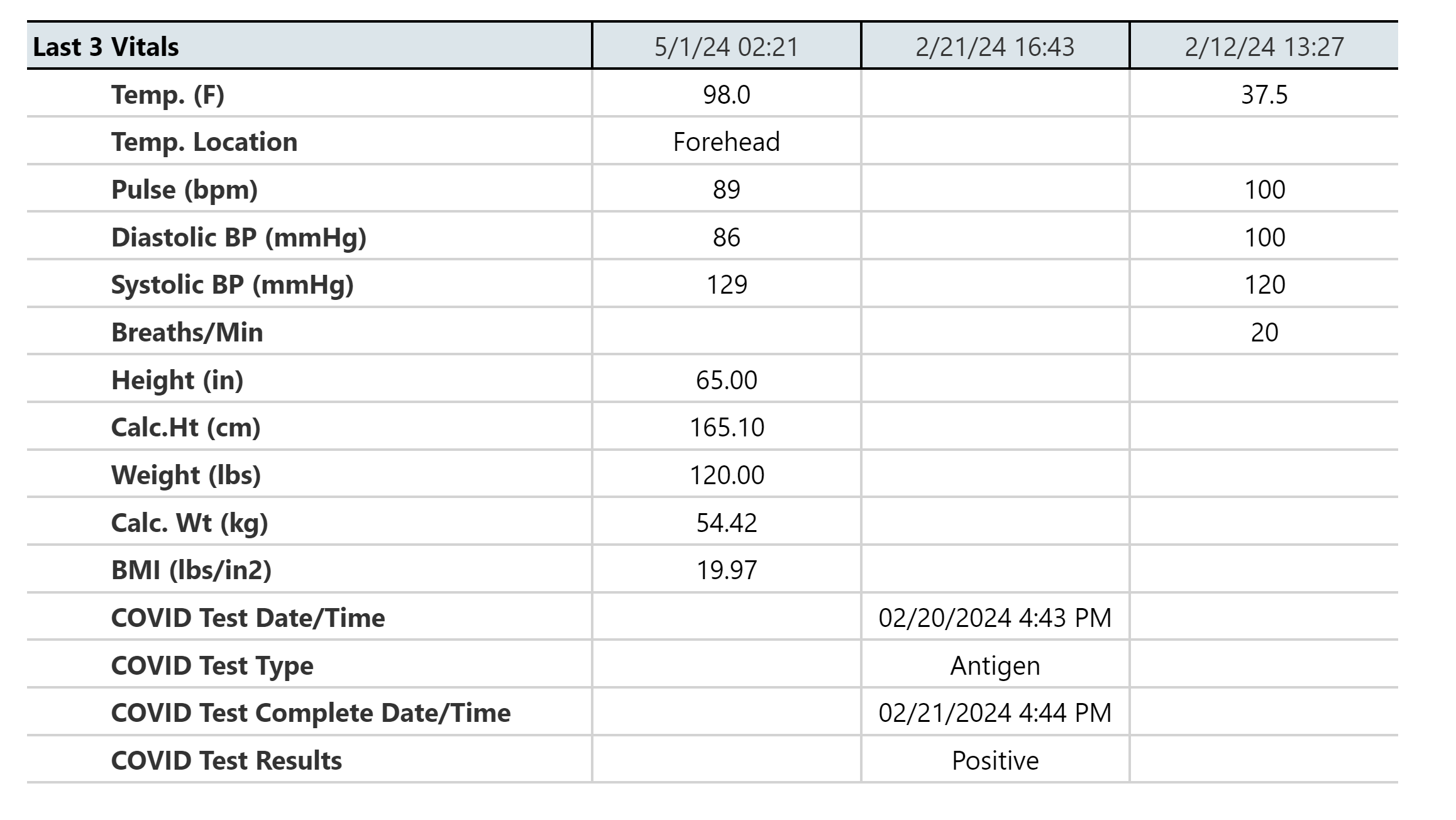
Last Vitals
This section will show the last three vitals that have been obtained for the patient.
Current Legal Status
This section will show any active legal statuses from Client Orders.

Conservators/Guardians
This will list any conservators (from dropdown choices) or guardians (from the checkmark boxes) listed from Client Information.
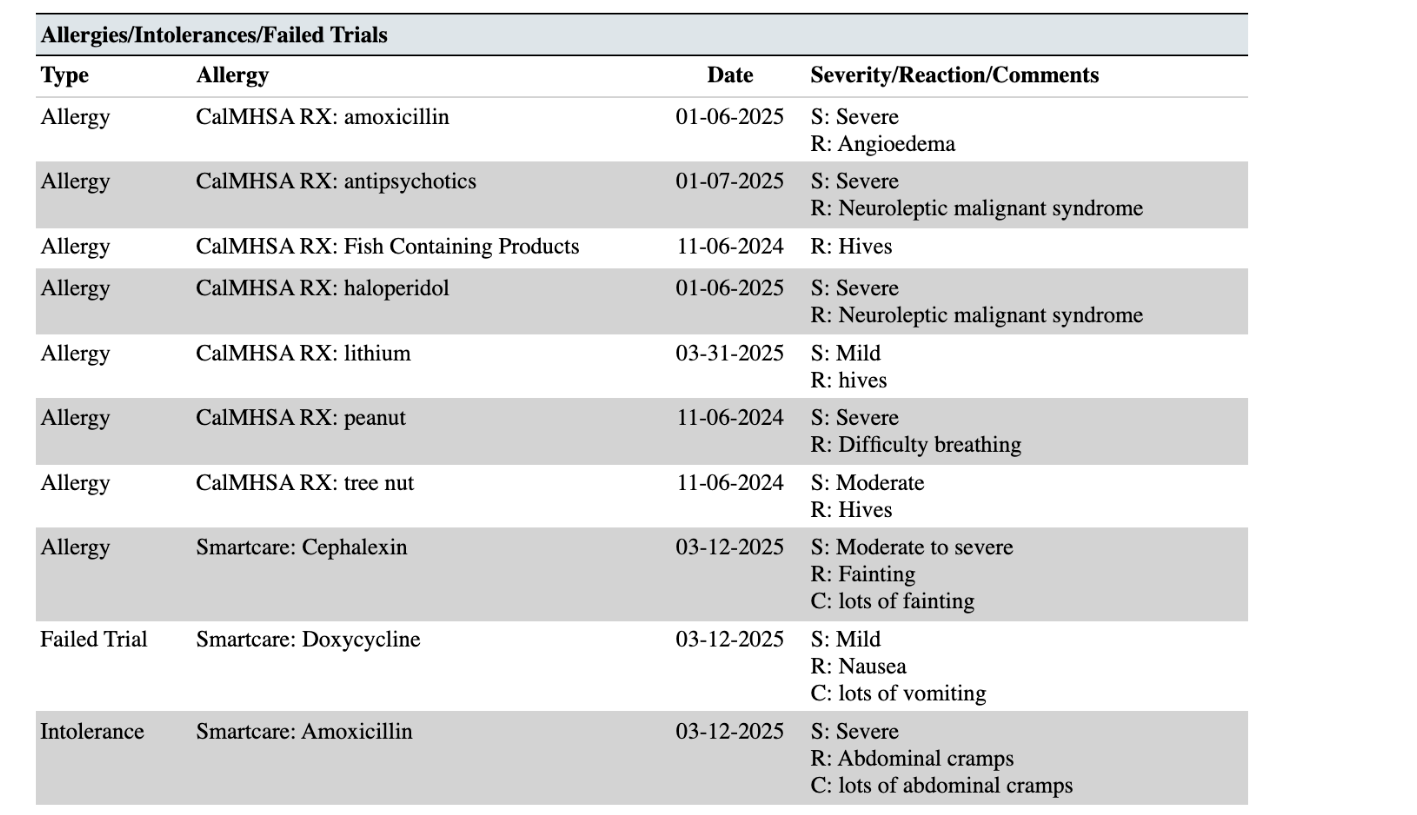
Allergies/Intolerances/Failed Trials
This will list any allergies from CalMHSA Rx and/or Smartcare Rx. It will provide information about when it was last modified, severity and the associated reactions. For Smartcare Rx allergens, it will list any also any failed trials or intolerances.
Note: If the same allergen (or NKDA/NKA) has been listed in multiple systems, then these will be listed as duplicates in this report, and there is no mechanism to capture any discrepancies.
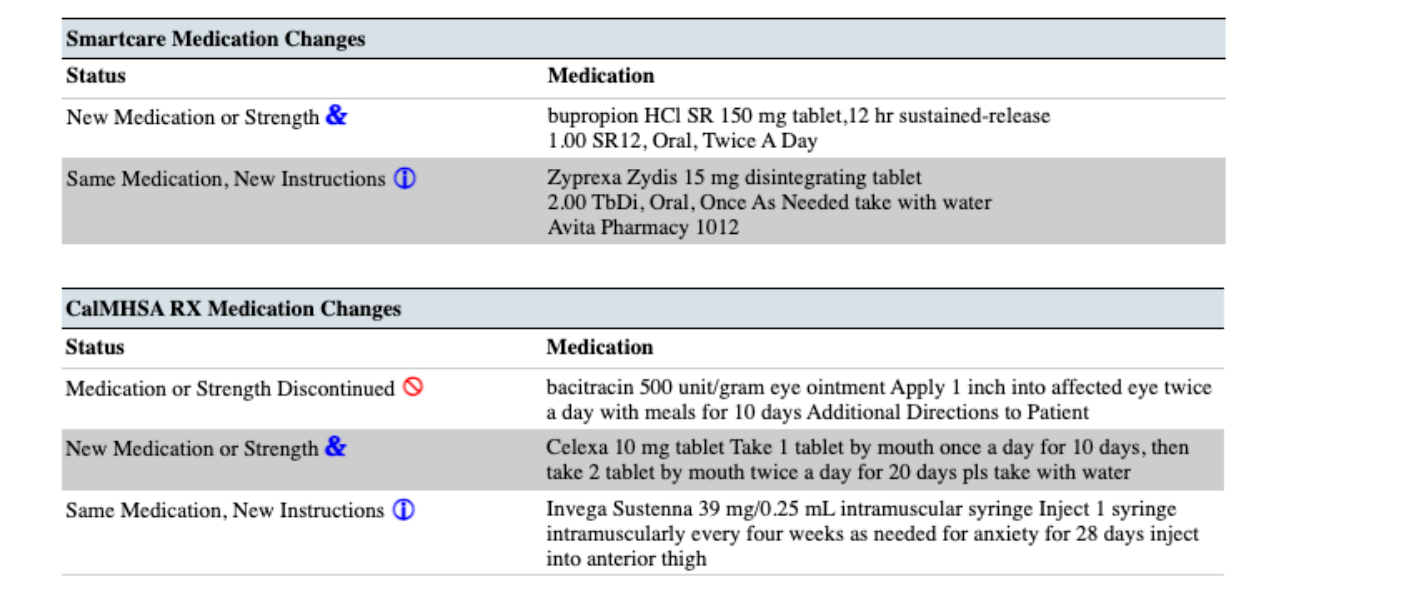
Medication Changes in the Last 24 Hours
This section will demonstrate the following changes that have been made to Medication Rx or to CalMHSA Rx within the last 24 hours. If there are any medications that have changed more than 24 hours ago that you need to highlight, this will have to be done manually. You can do this in the “CalMHSA Discharge Summary” or “CalMHSA Transfer Summary” within one of the text boxes such as “Discharge Plan” textbox.
Any medication that has been discontinued will be denoted by “Ø” in red.
Any medication which has been added, and/or a change in strength, will be denoted with a ”&” in blue.
Any medication that has new instructions and/or changes to the order sig will be denoted with a “i” in blue.
If there are no changes, there will be no icon.
Medications Ordered
In the Medication Ordered Section, this shows only current and active medications for CalMHSA Rx and SmartCare’s Client Orders/Medication Rx:
The transmission history will display only for Medication Rx medications and the icons will show up if:
- Green check mark =Successful transmission to pharmacy
- Red cross out = Error (e.g. rejection of transaction, prescription was not sent/received, unable to authorize)
- Blue paper icon = Printed/Faxed prescriptions
- Blue question mark icon = In queue/pending or other
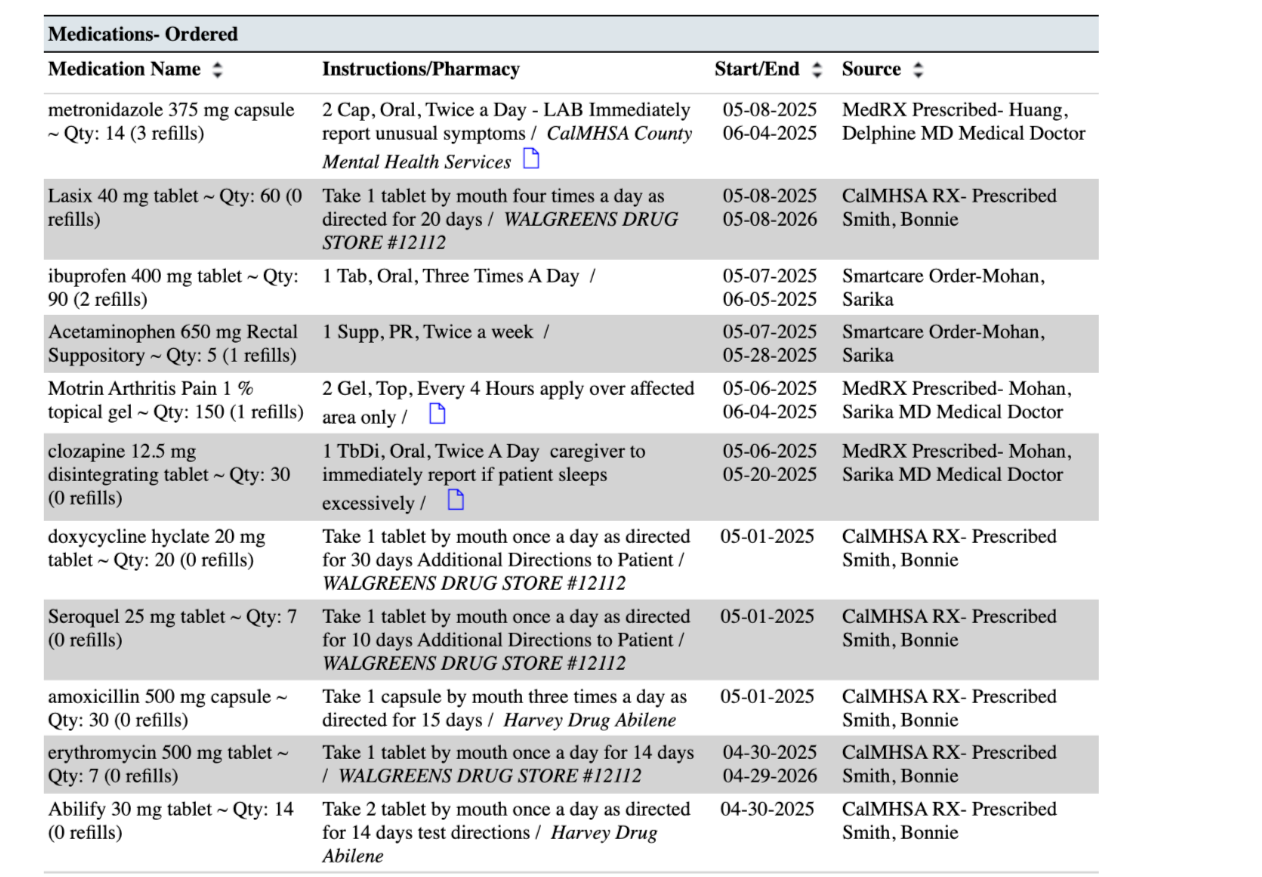
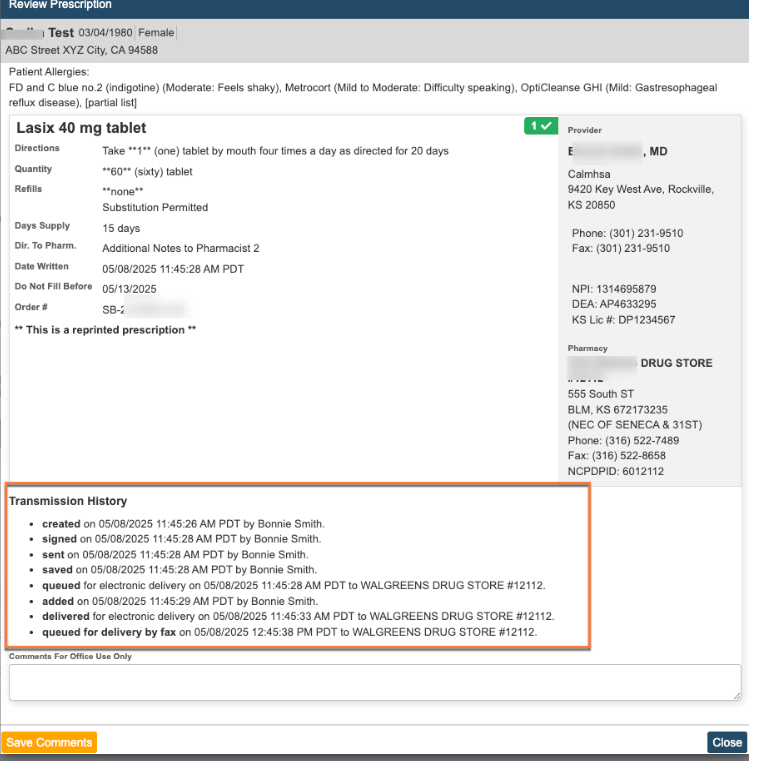
CalMHSA Rx medications ordered (prescriptions)– There are no icons for this group of medications within Face Sheet report. However, each prescription shows a detailed Transmission History under Review Prescription within Prescription Management in CalMHSA Rx system (screenshot below).
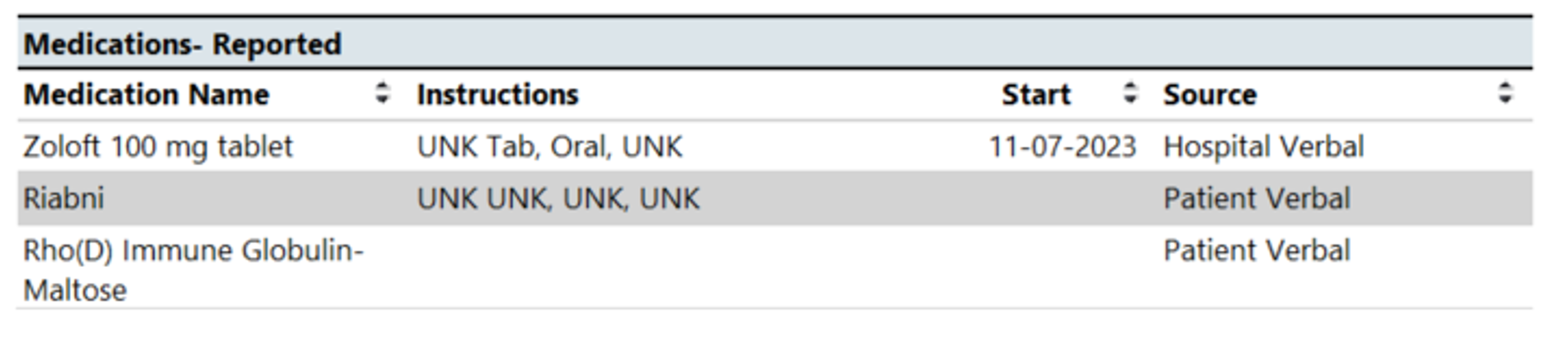
Medications-Reported
In the Medications Reported section, this shows only current and active medications that are reported by client or other external providers within Medication Rx Module.
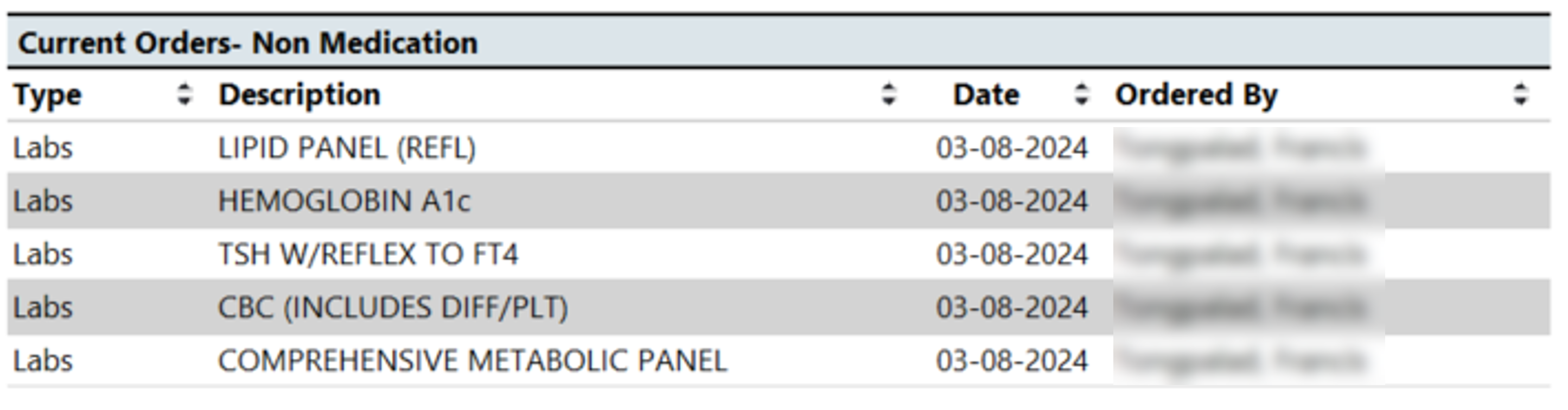
Current Orders-Non Medications
In the Current Orders Non- Medication section, this includes any “Active” or “Sent to Lab” orders within Client Orders with any type of order that is non-medication.
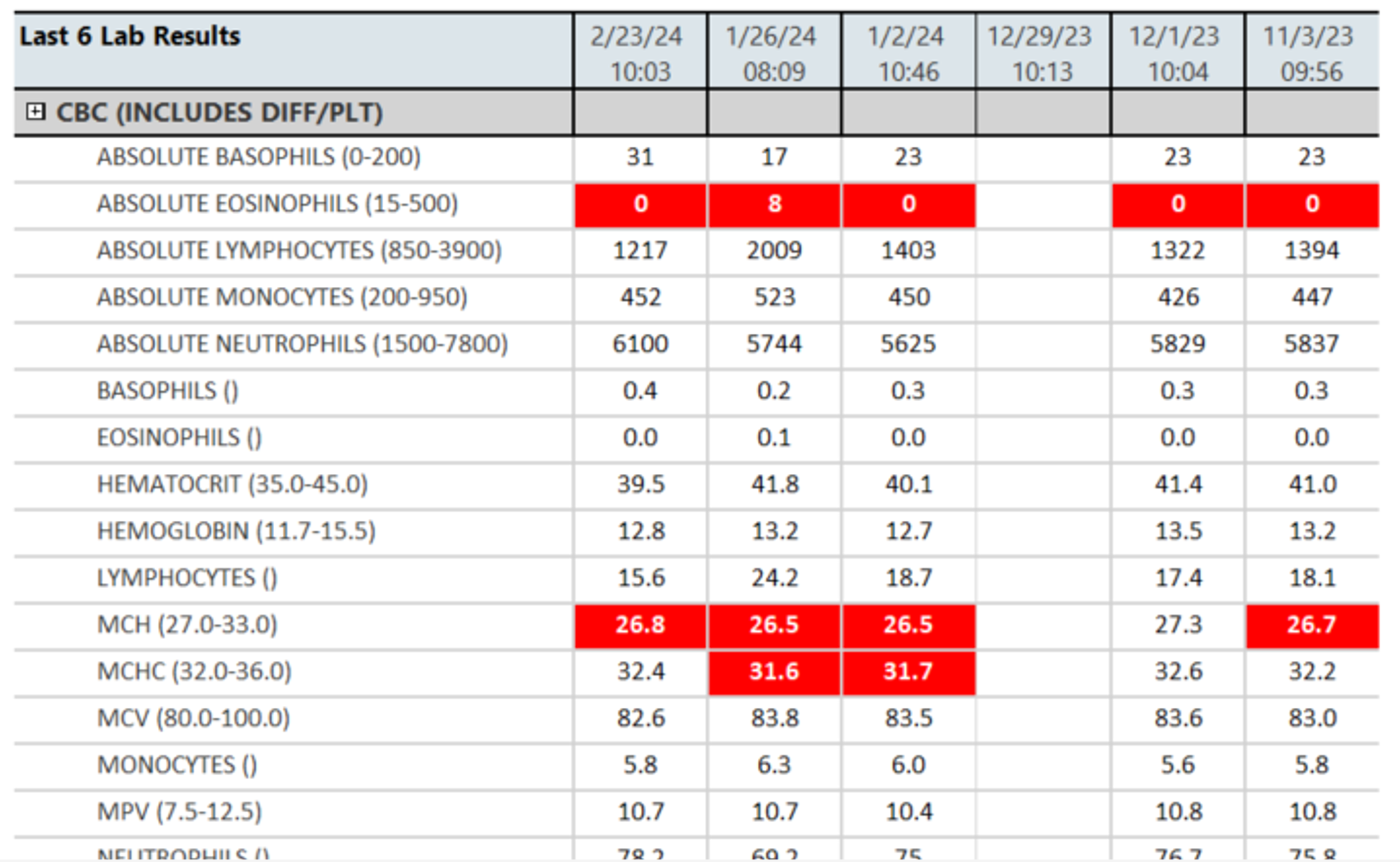
Lab Results
In the Lab Result section, this will show you any lab results for the client within the last 6 months. For any lab results in the gray section of any column, there will appear an “R” if it has been reviewed. For any lab value that has a ” * ” , if you hover over, it will show any lab vendor notes about that test or test result. For any lab value that is outside of the acceptable range, this will be highlighted in red. For more comprehensive lab results, one can use the “CalMHSA Cumulative Lab Flowsheet Report [Client]“.
Sections from CalMHSA Discharge Summary Document
If you want to create a new CalMHSA Discharge/ Transfer Summary Document, then please follow these instructions. Any saved text within these textboxes, and if selected in the filter parameters, will push into this report.
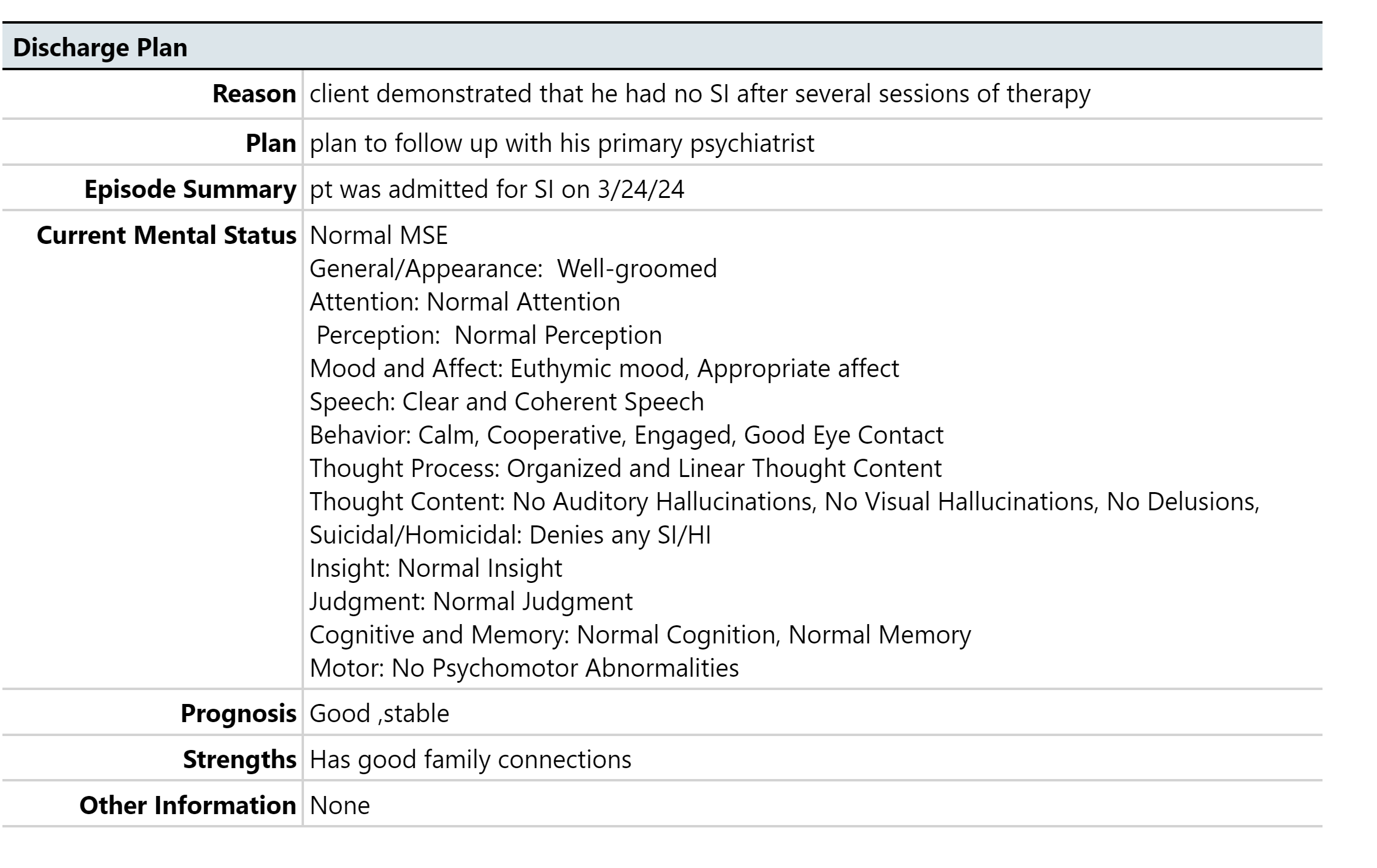
- DC/Trans Reason
- DC/Trans Plan
- DC/Trans Episode Summary
- DC/Trans Mental Status
- DC/Trans Prognosis
- DC/Trans Strengths
- DC/Trans Other Information
- Trans-Dietary
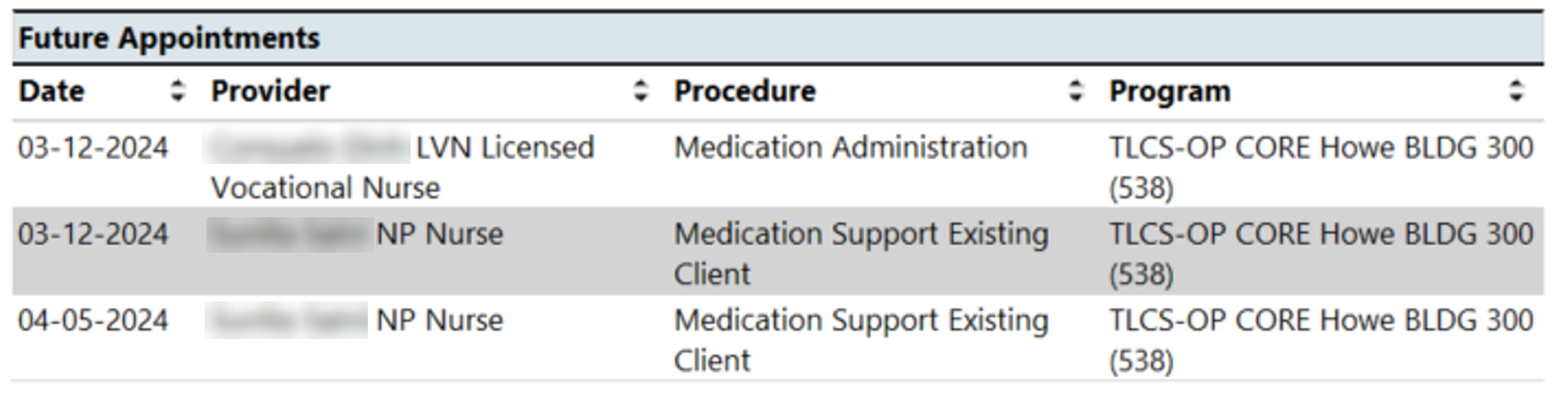
Future Appointments
In the Future Appointments section, this a compiled list of any future appointments that a client has scheduled within a CDAG.