The purpose of this report is to compile relevant client specific information that can assist in understanding a client’s medical history. It’s geared towards users in the inpatient or CSU setting. A client must be selected in order to run this report.
The defaulted users that have access to this are those with permission to the following roles:
- CalMHSA SysAdmin
- County Affiliate SysAdmin
- Medication Rx
- Medical Supervisor
- Nurse Medical IP/CSU/Res
- Prescriber
- Prescriber IP/CSU/Res
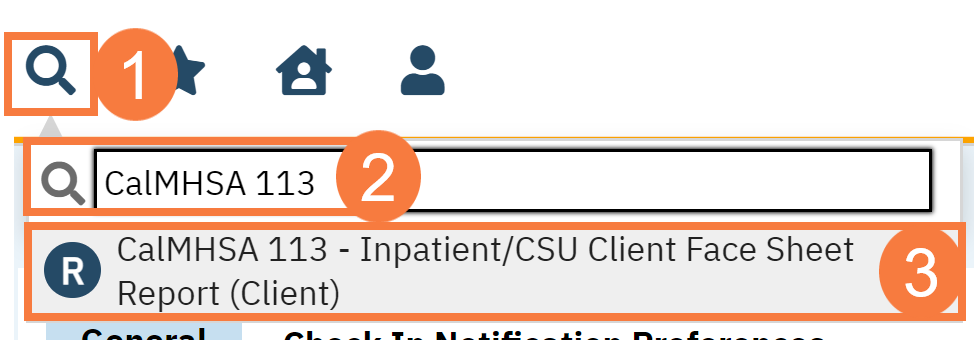
- With a client open, click the Search icon.
- Type CalMHSA 113 in the search bar.
- Click to select CalMHSA Client Medical Face Sheet Report (Client).
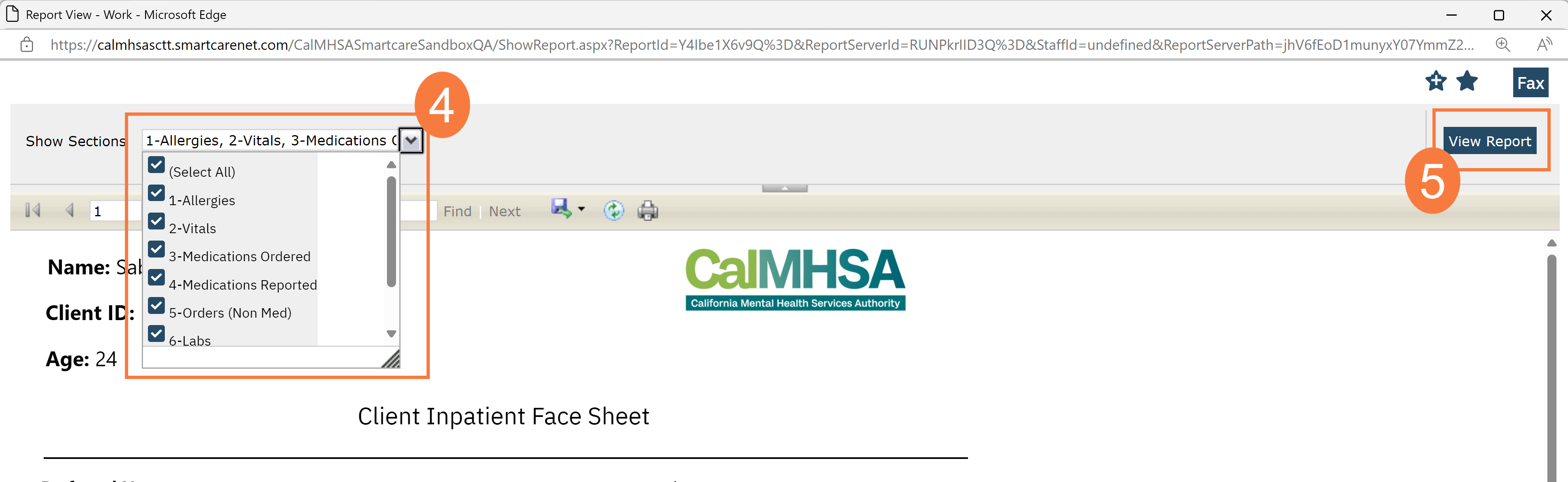
- The report window will open. Click the show sections menu drop-down and unselect the fields you don’t want on the report.
- Click View Report to update the report.
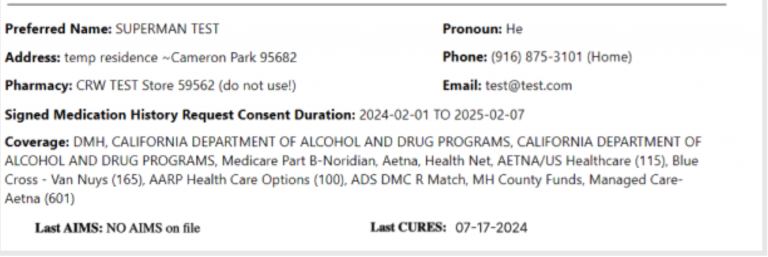
Patient Demographics
This information is pulling from the Client Information screen. In addition to this information, it will pull in the following:
- Signed Medication History Request Consent Duration: This will pull into the document if the patient has signed the consent to allow for you to view Surescripts and the date they provided consent.
- Pharmacy: This pulls the pharmacy information as entered in SmartCare.
- Coverage: The client’s insurance coverage will appear here.
- Last AIMS and Last CURES: This data is pulling from the Psych/Medical Note template when the provider checked off that they reviewed or completed these tasks.
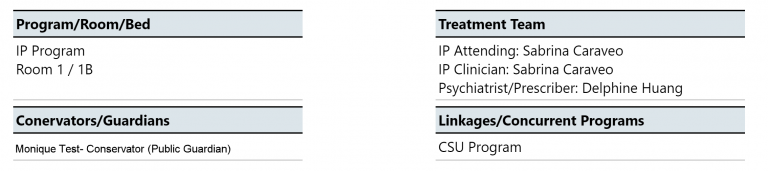
- Program/Room/Bed: This will give information about the patient’s current program and bed assignment.
- Treatment Team: This will list the provider(s) and their title listed in the Treatment Team screen.
- Conservator/Guardian: This will list any conservators (from dropdown choices) or guardians (from the checkmark boxes) listed from Client Information.
- Linkages/Concurrent Programs: This will list any concurrent and active programs that the patient is also enrolled in and their last “show” date
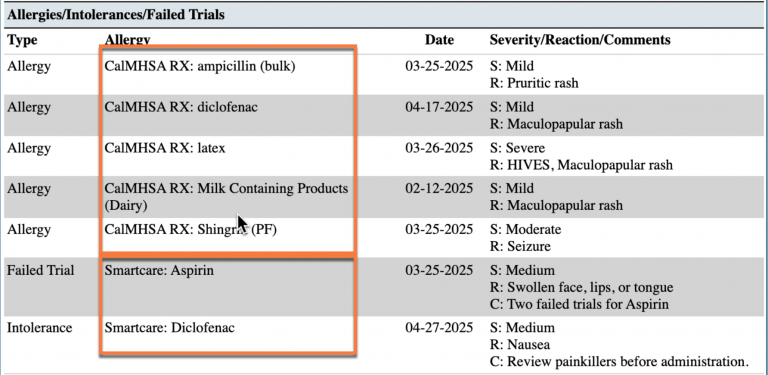
Allergies
- “S” refers to severity of the reaction
- “R” refers to reaction to the drug/allergen
- “C” is any comments that was documented
- Each allergen will also list which e-prescribing system this information came from (e.g. SmartCare, CalMHSA Rx). This is displayed in the column title ‘Allergy’.
- “NDKA” will be used if there are no known allergies.
- If there are no previous record marked, then “Allergies have not been set up for this client yet” will appear to remind provider that for this patient, this task has not been completed.
- SmartCare allergies will also display their associated allergy type (e.g. Allergy, Intolerance, Failed Trial), and, if there are any comments.
- Date – This information in the Allergies section is derived from “ModifiedDate” for SmartCare and “LastModifiedDate” for CalMHSA Rx, respectively.
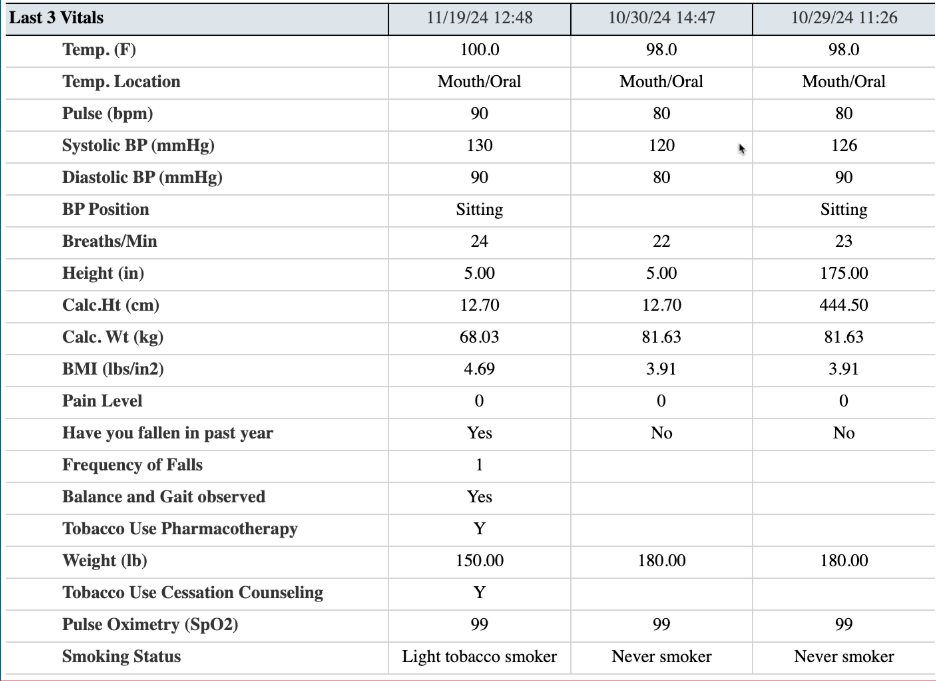
Vitals
In the Vitals section, you will be able to see the last 3 sets of vital signs. This will allow you to see a range of vitals over a period of time.
Medications Ordered
In the Medication Ordered Section, this shows ONLY current and active medications in CalMHSA Rx and SmartCare’s Medication Management Rx (depending on which Rx module is used) and from Client Order.
SmartCare Medication Management Rx Medications and those from Client Orders– The following icons will show up for Medications ordered in SmartCare Medication Management Rx if:
- Green check mark =Successful transmission to pharmacy
- Red cross out = Error (e.g. rejection of transaction, prescription was not sent/received, unable to authorize)
- Blue paper icon = Printed/Faxed prescriptions
- Blue question mark icon = In queue/pending or other
Examples below:
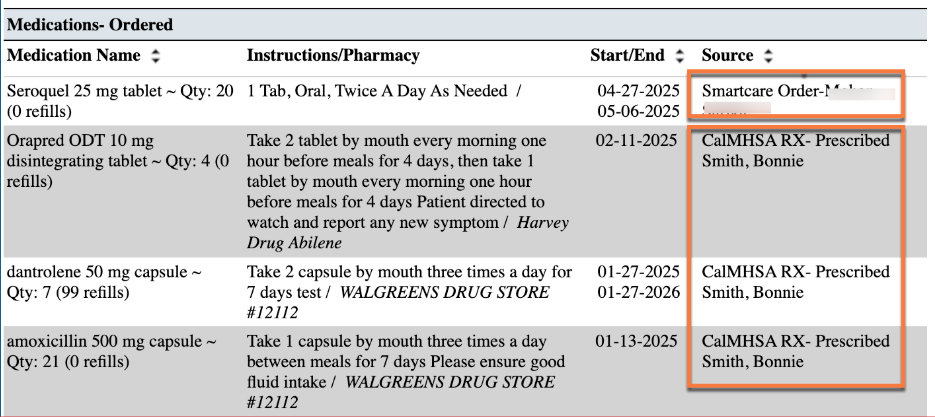
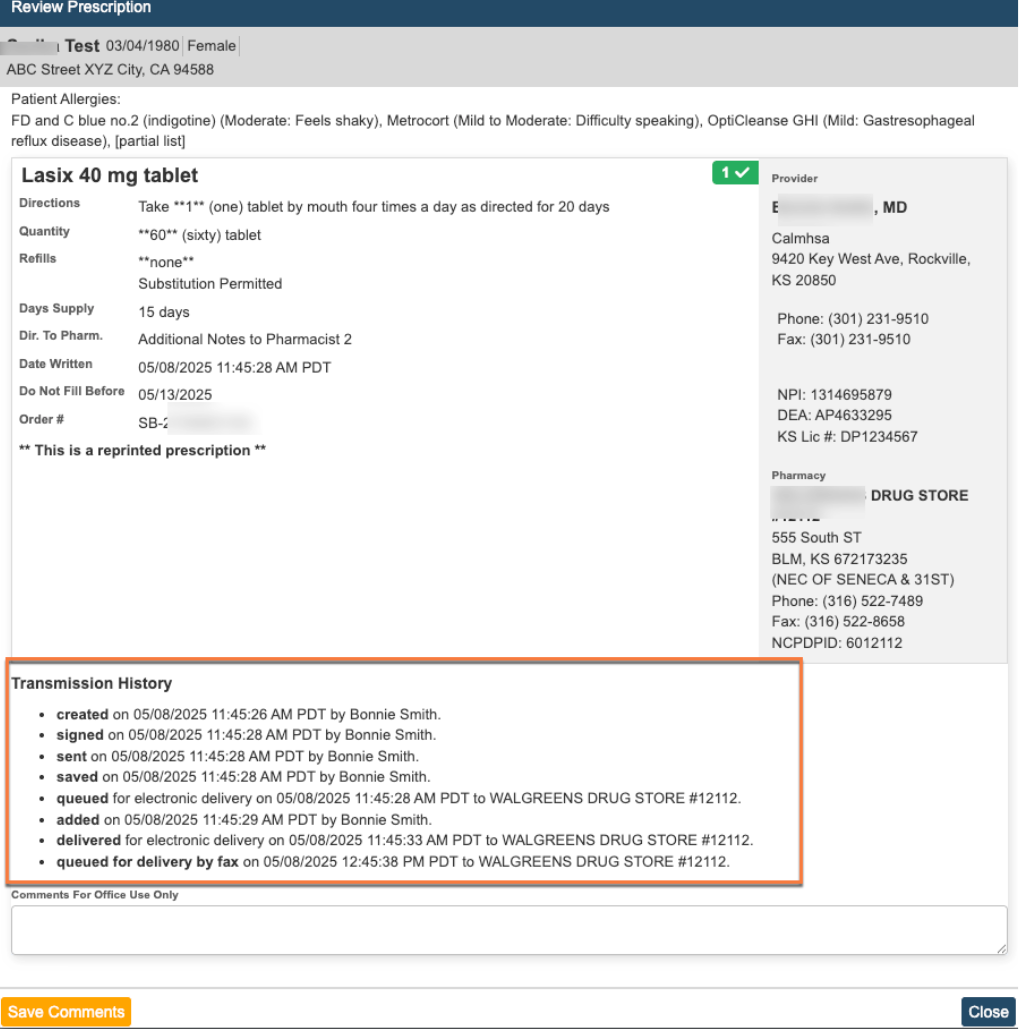
CalMHSA Rx medications ordered (prescriptions)– There are no icons for this group of medications within Face Sheet report. However, each prescription shows a detailed Transmission History under Review Prescription within Prescription Management in CalMHSA Rx system (screenshot below).
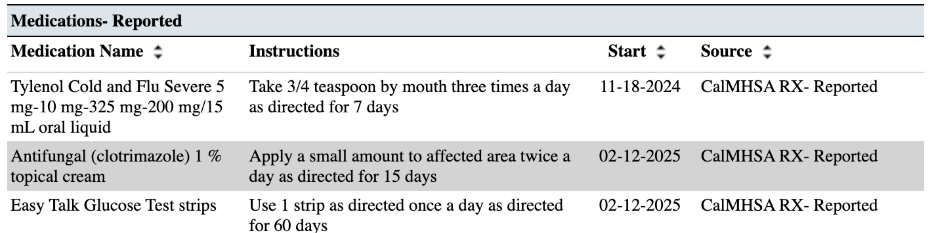
Medications-Reported
In the Medications Reported section, this shows ONLY current and active medications that are reported by client or other external providers within Medication Management Rx or CalMHSA Rx Module. Look at screenshots below that display information being pulled into the Face Sheet from Rx modules
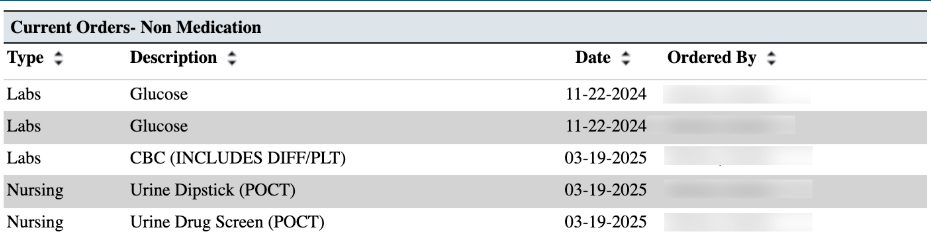
Current Orders-Non Medications
In the Current Orders Non- Medication section, this includes any “Active” or “Sent to Lab” orders within Client Orders with any type of order that is non-medication.
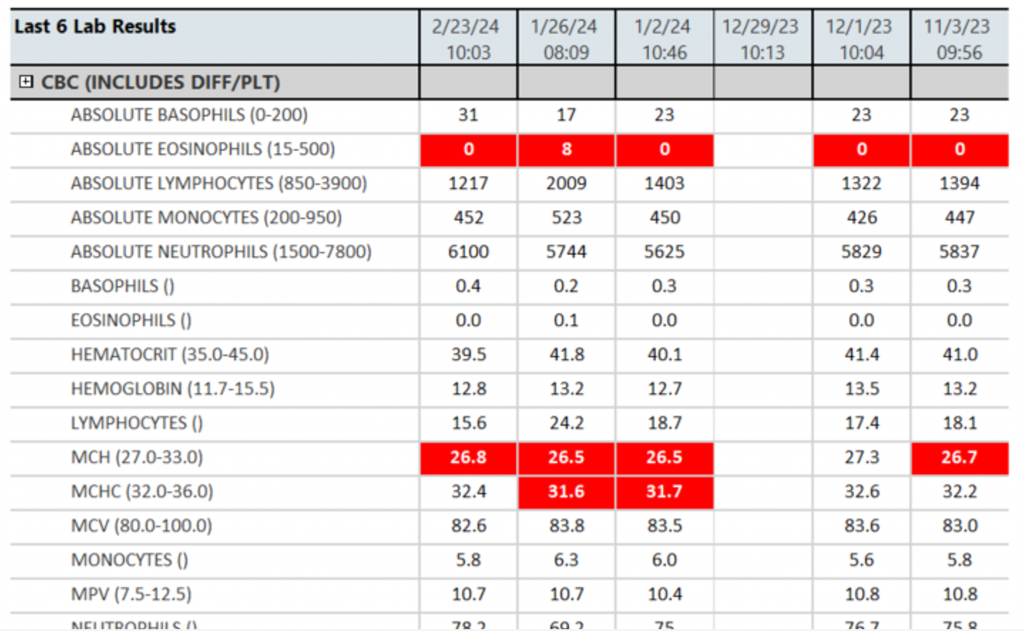
Lab Results
In the Lab Result section, this will show you any lab results for the client within the last 6 months. For any lab results in the gray section of any column, there will appear an “R” if it has been reviewed. For any lab value that has a ” * ” , if you hover over, it will show any lab vendor notes about that test or test result. For any lab value that is outside of the acceptable range, this will be highlighted in red. For more comprehensive lab results, one can use the “CalMHSA Cumulative Lab Flowsheet Report [Client]“.
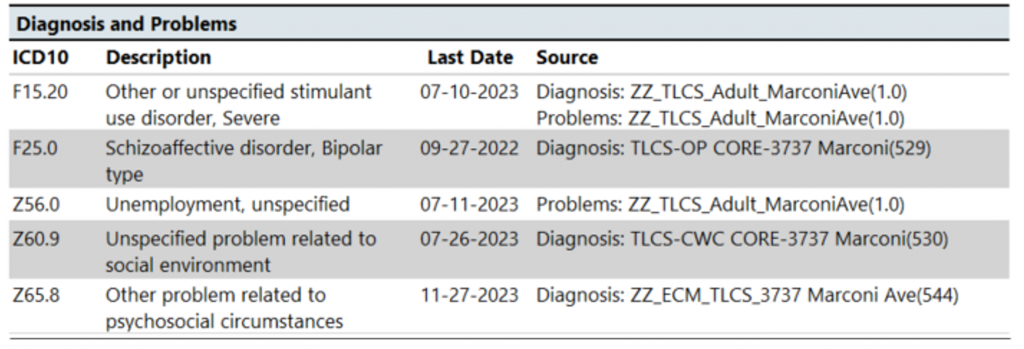
Diagnosis and Problems
In the Diagnosis and Problems section, this is a compiled list of any diagnosis and /or problems that share the same ICD10 codes within a CDAG. It will also list the source of the information (whether it comes from Diagnosis Document or from the Client Problem List) as well as the program. The last date refers to the last time this information was updated.
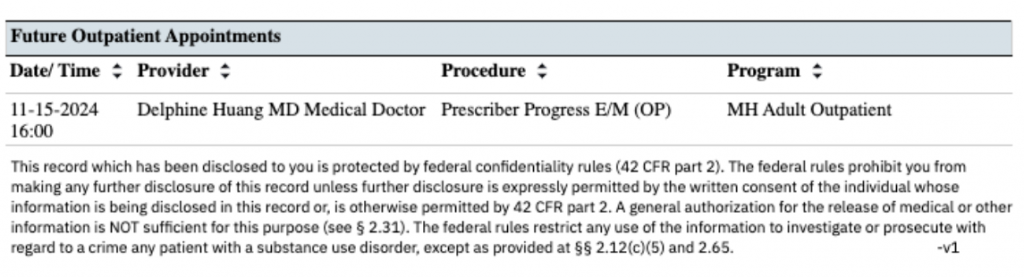
Future Out-Patient Appointments
In the Future Appointments section, this a compiled list of any future appointments that a client has scheduled within a CDAG.