This document is to create a safety plan with and/or for the patient to prevent seclusion and/or restraints. For some users, it can be helpful to generate key phrases to be more efficient.
This document will initialize data from the most recently signed document. This document will also allow different authors to initialize off the last version. It is program specific and it is NOT visit episode based. If there needs to be a blank version, then user will need to delete the section’s existing text manually.
There is a general safety plan available and instructions can be found here.
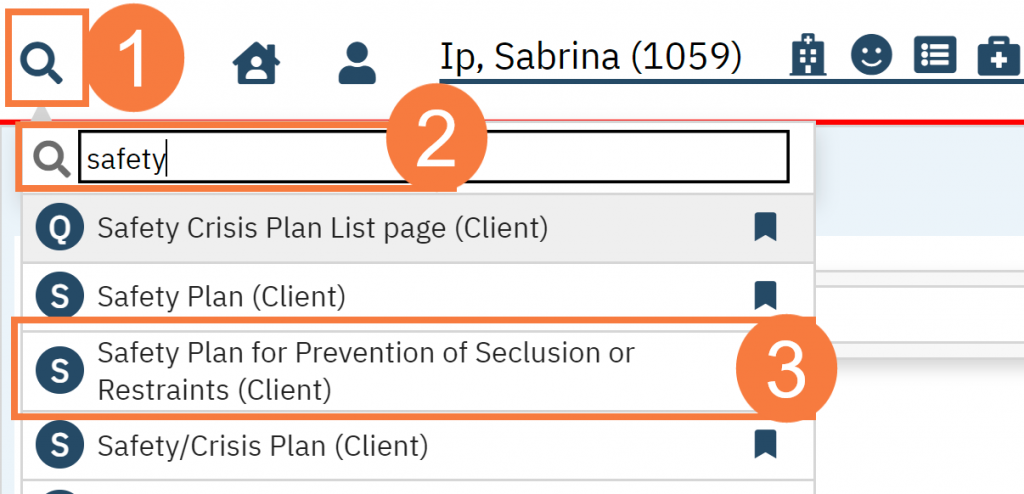
- Click the Search icon.
- Type Safety Plan in the search bar.
- Click to select Safety Plan for Prevention of Seclusion or Restraints (My Office)
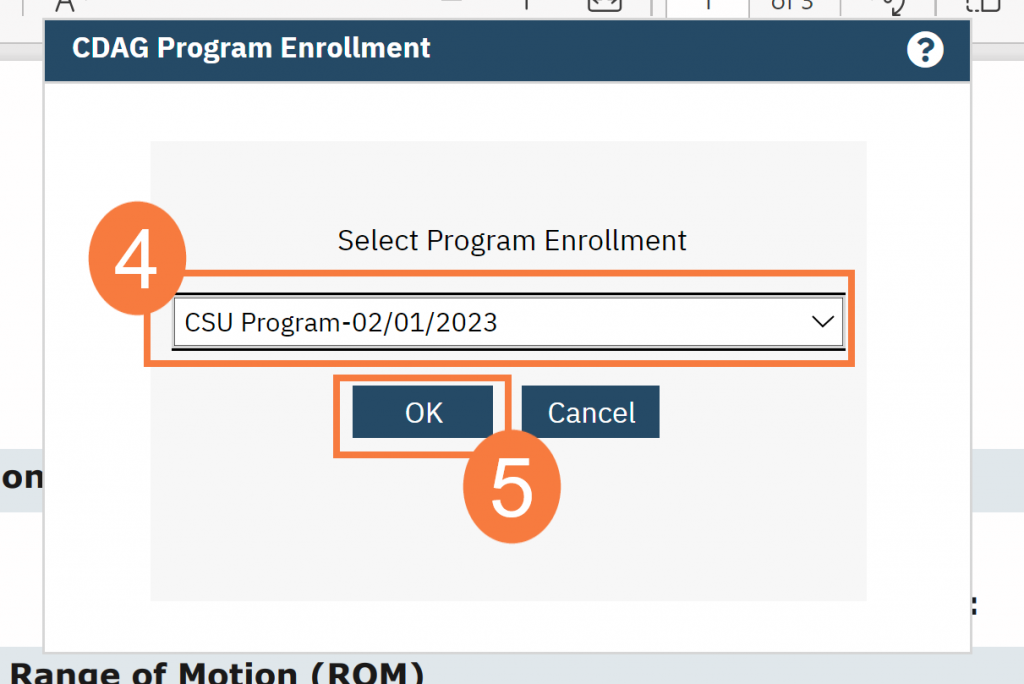
- In the CDAG Program Enrollment window, click to select the appropriate program.
- Click OK.
Note: This document is set up to pull in the last Safety Plan that was created for this patient if within the same program, regardless of author. This was created so that if multiple safety plans are created within a visit episode, this would minimize the need to rewrite. That said, if patient is readmitted then a user may need to manually clear the fields that are no longer relevant.
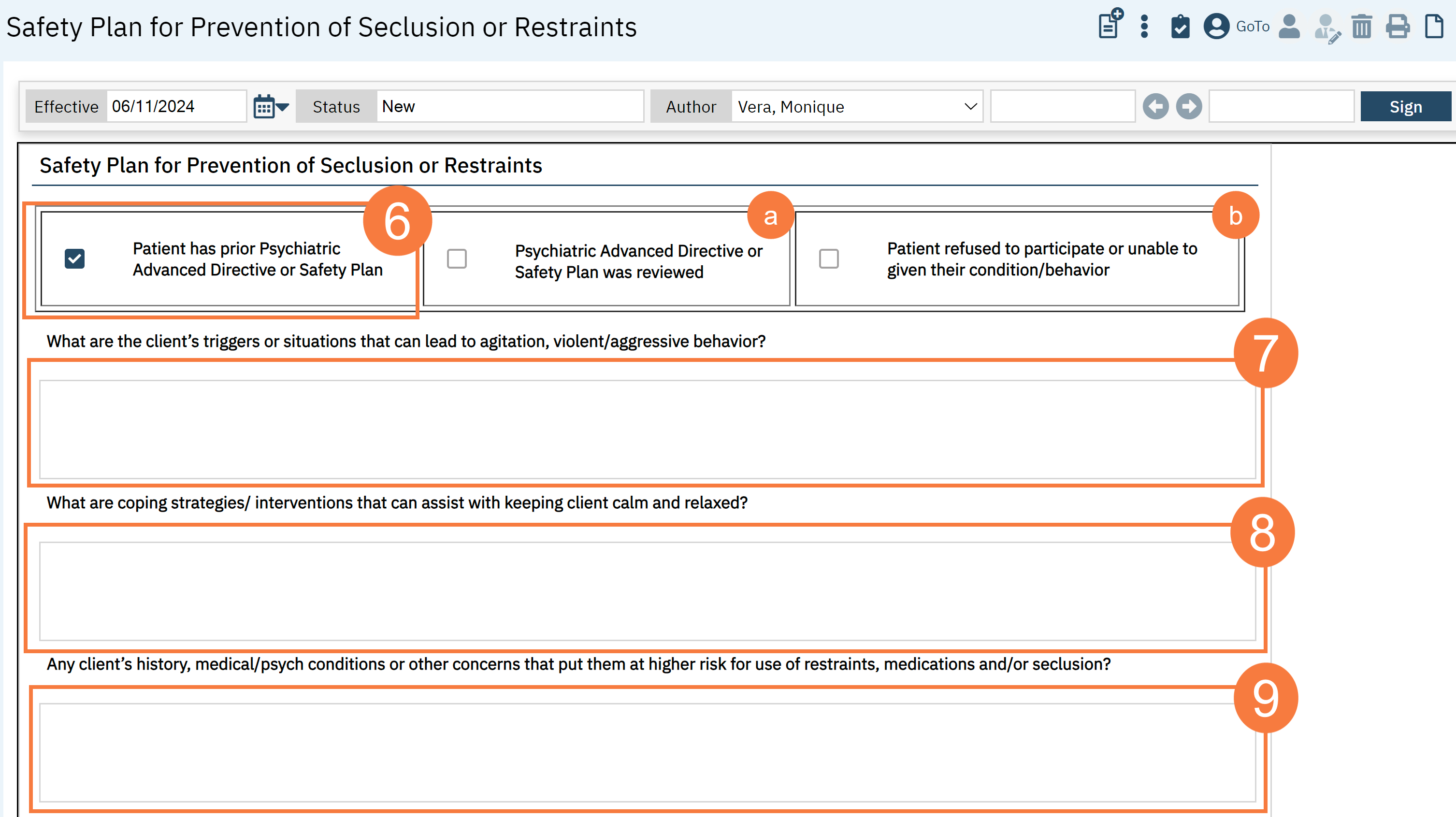
- Checkmark if there is a prior Psychiatric Advanced Directive or Safety Plan
- A subsequent question will appear, asking if the “Psychiatric Advanced Directive and/or Safety Plan has been reviewed yet.” Checkmark, if relevant.
- If the patient refused to participate or you are unable to complete because of their condition/behavior, you can indicate with a checkmark.
- Describe what are the client’s triggers and/or situations that can lead to agitation or violent/aggressive behavior? This is a mandatory field.
- Describe what are the coping strategies or interventions that can assist in avoiding seclusion and/or restraint by keeping the client calm and relaxed? This is a mandatory field to fill out.
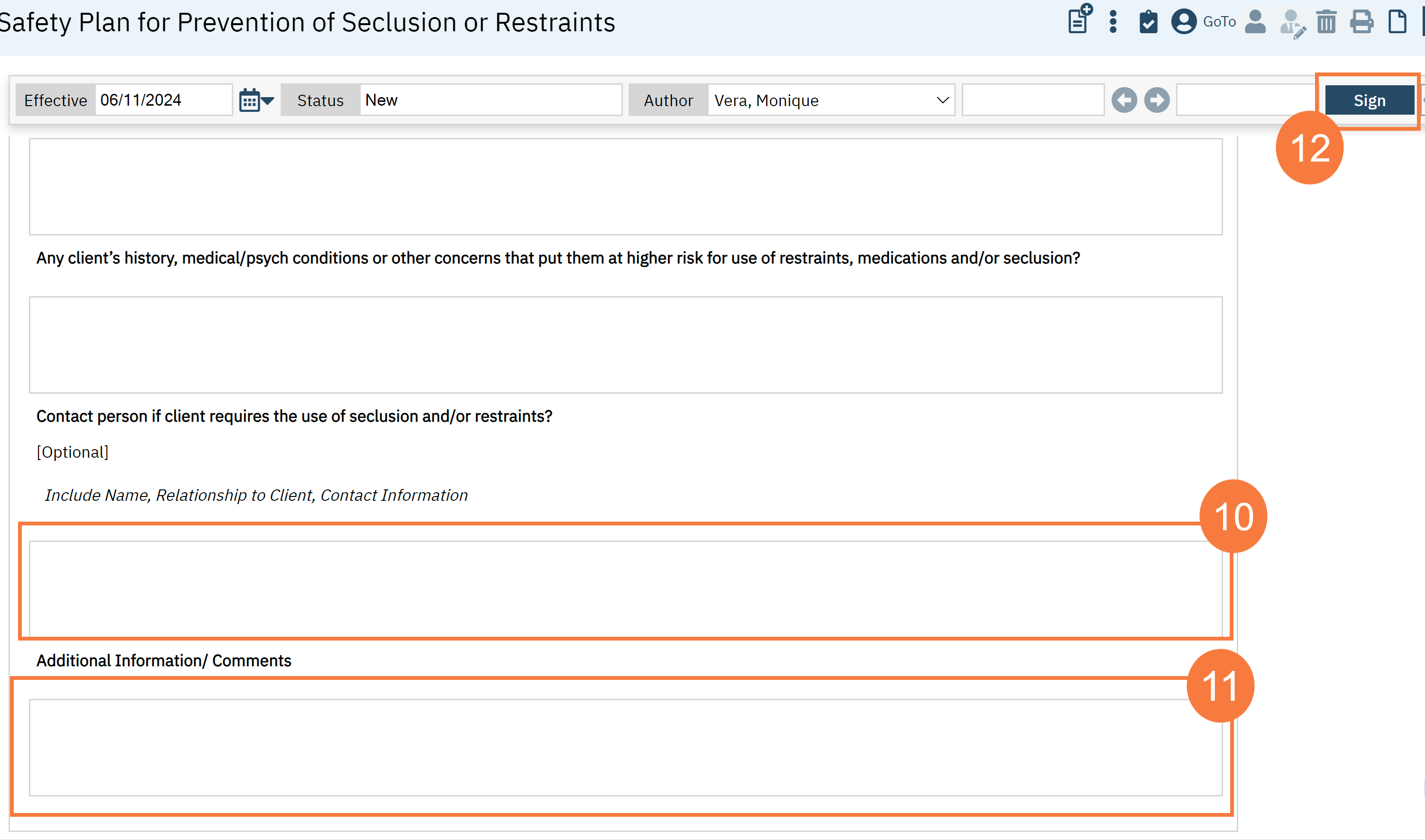
- Document any concerns that would put the patient at risk for the use of restraints, involuntary emergency medication and/or seclusion.
- If the patient has a contact person or patient advocate that should be contacted in the event of a seclusion or restraint episode, please record the name, relationship to the client, and client information.
- Describe any additional information or comments .
- Click Sign.