UPDATE Jan 2026: CARE Act Data Dictionary v2.0 is now in production environments.
Overview
The Community, Assistance, Recovery, and Empowerment (CARE) Act is a California State initiative designed to create a new pathway to deliver mental health and substance use disorder services to some of the most vulnerable people. This initiative involves court processes to help connect community members with severe behavioral health issues.
Health Management Associates (HMA), is a consulting firm that is managing the statewide implementation of the CARE Initiative. Their website, https://care-act.org, provides a wealth of information, including training videos, downloadable resources, and FAQs.
DHCS also has a site dedicated to the CARE Act, https://www.dhcs.ca.gov/Pages/CARE-ACT.aspx, which includes legislation references, related information notices, data dictionaries, and statewide reports.
Behavioral Health Plans (BHP), otherwise known as county behavioral health departments, have a key role in the CARE process. They help assess referred or petitioned individuals for eligibility and connect CARE participants to needed services.
The CARE process is a court process and is separate from treatment services. In some counties, CARE staff may also provide treatment services, though the BHPs requirement under CARE is to coordinate and connect the participant with treatment providers, rather than providing treatment directly. CARE staff have specific CARE process activities they deliver, which are not claimed to Medi-Cal. CARE staff may also be required to write official documents for the courts, or be asked to sign court documents as part of the CARE process.
This protocol is meant to help convey how CalMHSA has helped to set up SmartCare to assist BHPs in their implementation of CARE Act.
Privacy Re: Court Documents
Since the CARE Act includes creating and receiving of court documents, there is some concern about privacy, as these documents are not often managed in the same way as mental health or substance use treatment records. CARE Act pilot counties indicated that sequestration of these documents from the client’s medical record is preferable.
In SmartCare, all documents will show on the “Documents (Client)” list page, within CDAG limitations. There was concern that even if a client agreed to share their medical records with all the providers in SmartCare via a consent to share confidential information, court documents may not be included in that authorization. For this reason, CARE Act documents should be restricted to only CARE Act program staff. This is managed in SmartCare by the “CARE Act Add-On” user role. Staff who work in the CARE Act program and will need to be able to see court documents related to CARE Act clients should be assigned this user role in additional to their standard base user role. See User Role Overview for more details about permissions and user roles.
All CARE Act documents should be created under the CARE Act program(s) within your system. This program should be added to appropriate CDAGs based on your county’s framework.
With these two items, program/CDAG and user permissions, BHPs should be able to set up their SmartCare instance to address privacy concerns. For example, a county may determine it is beneficial for service providers to be able to see CARE Act program information (e.g. client appointments, hearing dates, CARE Act treatment team members, etc.) to coordinate care, but not allow service providers to be able to see the documents that the CARE Act staff create. By using both CDAG and use roles, this is possible.
CARE Act Activities and Reimbursement
BHIN 24-015 provides a list of activities, and their definitions, that are associated with the CARE Act initiative that can be reimbursed. These include:
- Court Hearing Time
- Court Report
- Outreach and Engagement
- Notice
- Data Reporting
One activity not included in the BHIN is CARE Act Implementation activities, such as meetings with stakeholders, creation of policies and procedures, and development time spent on forms and record tracking methods. CalMHSA feels it’s important for BHPs to keep track of this activity as well, even if it isn’t reimbursable.
CalMHSA has created procedure codes and calendar event types to track these 6 activities in SmartCare (5 from the BHIN and 1 for implementation activities). Service Notes should be used for activities related directly to CARE Act clients while calendar events should be used for general activities that aren’t tied to a specific client, such as gathering and submitting state reporting files.
The SmartCare Staff Calendar only has records for users who are considered “clinicians”. This means that administrative support staff, including receptionists, medical records, billing, and quality assurance staff, will likely not have a SmartCare calendar where they can document their activities. CalMHSA recommends that BHPs use another method for tracking CARE Act activity time spent by these staff members.
Service notes include the ability to account for travel time and documentation time associated with the service. Users should always enter any travel and documentation time in these fields, even if they are not reimbursable. This provides BHP leadership with important service data. DHCS has indicated that travel time is reimbursable for Outreach and Engagement activities with regards to the CARE Act, so any travel time entered in the service for this activity will be included in the reimbursable time.
CARE Act pilot counties indicated that they needed to be able to track specific actions at different types of CARE Act hearings, such as whether the client was present, if the judge made a determination, etc. CalMHSA therefore created custom CARE Act procedure codes for each hearing type along with custom progress notes for to help track data relevant to each type of hearing.
Below is a list of the procedure codes and calendar event types that CalMHSA has created for CARE Act activity tracking and reimbursement. Please note that none of these procedure codes are considered “billable” codes, as the reimbursement process for CARE Act is not the same as claiming to Medi-Cal.
- Procedure Codes
- CARE Act – Hearing Time Activity (CARE Act Narrative Note)
- CARE Act – 1 Year Status Reviewing Hearing (CARE Act 1 Year Status Review Hearing Note)
- CARE Act – CARE Plan Review Hearing (CARE Act Plan Review Hearing Note)
- CARE Act – Case Management Hearing (CARE Act Case Management Hearing Note)
- CARE Act – Evaluation Review Hearing (CARE Act Evaluation Review Hearing Note)
- CARE Act – Graduation Hearing (CARE Act Graduation Hearing Note)
- CARE Act – Hearing on Deferred Ruling (CARE Act Hearing on Deferred Ruling Note)
- CARE Act – Hearing on the Merits (CARE Act Initial Hearing Note)
- CARE Act – Initial Hearing (CARE Act Initial Hearing Note)
- CARE Act – Progress Review Hearing (CARE Act Progress/Status Review Hearing Note)
- CARE Act – Status Review Hearing (CARE Act Progress/Status Review Hearing Note)
- CARE Act – Court Report Activity (CARE Act Narrative Note)
- CARE Act – Outreach and Engagement (CARE Act Narrative Note)
- CARE Act – Notice Activity (CARE Act Narrative Note)
- CARE Act – Data Reporting (CARE Act Narrative Note)
- Calendar Events Types
- CARE Act – Data Reporting
- CARE Act Implementation Time
Reimbursement Process
The reimbursement process involves submitting an invoice on DHCS’s template, which can be found on DHCS’s website. CalMHSA has created a CARE Act Claiming Report that will provide you with information required to complete the DHCS reimbursement form. This report will collect all reimbursable time for each reimbursable activity, including travel time for outreach and engagement. This time is rounded to the nearest 0.25 hours, per DHCS guidance. The BHP will need to merge data from SmartCare and external tracking methods to ensure all CARE Act activity time is properly invoiced.
Inquiries about CARE Act
SB 1400 expanded the initial CARE Act to include tracking information about inquiries received about the CARE Act process. The Data Dictionary version 2.0 includes specific data points for tracking “CARE Act Inquiries”.
In SmartCare, these are tracked via the Inquiries process. CalMHSA has added values to existing Inquiry Details fields to allow counties to easily document CARE Act inquiries. See How to Document a CARE Act Inquiry for details. CalMHSA also created the “CalMHSA 807 – CARE Act Inquiries Report” for counties to use during quarterly state reporting submissions.
Note: Streamline later created a separate tab for CARE Act Inquiry tracking and reporting. CalMHSA is not currently using the CARE Act Inquiry tab, as the existing report uses the General tab on the Inquiry Details screen. Counties may test this feature in their QA systems if desired. CalMHSA will continue to test and will recommend a change if and when it becomes prudent.
CARE Act Process
CARE Act System Referrals
SB 1400 expanded the initial CARE Act to include “System Referrals”. These are referrals made by specific facility or program types (MIST, FIST, AOT, and LPS Facilities) and are sent to BHPs. BHPs then have 14 business days to complete an assessment. The BHP can attempt to engage the client in voluntary treatment. If the BHP determines that the client meets (or is likely to meet) CARE Act criteria and isn’t engaging in voluntary treatment, the BHP will submit a CARE Act petition for the client.
Some of these facilities may use the county’s instance of SmartCare as their EHR. For this reason, CalMHSA has created a CARE Act System Referral document in SmartCare, based on the State’s template provided with BHIN 25-012. Completing this document does not automatically enroll the client in the SmartCare CARE Act Program. Follow the referral workflow of entering the client in “Requested” status in the CARE Act Program. See How to Document a CARE Act Referral (DD 2.0) for details.
When a BHP receives a referral, they should create the person as a client in SmartCare, if not already a client, and enroll the client in the CARE Act program. They should also create a CARE Episode document to record this referral. This connects the client to the CARE Act for multiple tracking purposes. The CARE Act staff should document all assessment and outreach and engagement activities in the CARE Act program using the procedure codes mentioned in the CARE Act Activities section above. If the CARE Act team determines the client should be petitioned, they should use the State form. The petition is not a SmartCare document, but the finished petition should be uploaded to the client’s chart. Regardless of the decision to petition or not, the BHP must include this referral in the state reporting. See How to Document a CARE Act Referral (DD 2.0) for details.
Steps to take when you receive a CARE Act System Referral:
- Check to see if the individual is a client. If they aren’t, create them as a client in SmartCare using the Inquiry process.
- Enroll the client in the CARE Act program. You will use this program for all CARE Act related documents and services for this client.
- Scan/upload the CARE Act System Referral to the client’s chart. Use “Client (Medical Records)” with Record Type = “CARE Act System Referral (scanned)”.
- Create a CARE Episode document to record the referral information.
- Document all activities in the CARE Act program using the appropriate CARE Act Activity procedure codes.
- Complete state reporting requirements.
Steps to take when you determine the referred client should be petitioned:
- Complete the petition form (CARE 100), which can be found on the State’s website, and submit per your county’s process.
- Upload the petition to the client’s chart in SmartCare. Use “Client (Medical Records)” with Record Type = “CARE Act Petition (scanned)”.
- Continue to document all activities in the CARE Act program using the appropriate CARE Act Activity procedure codes.
- Continue to complete state reporting requirements.
CARE Act Petitions
The CARE Act historically has focused on “petitioned individuals”, meaning community members who have been petitioned as a potential CARE Act participant. These petitions go to the court, who holds hearings to determine if the petitioned individual meets CARE Act criteria or not. The court may request the BHP to do a formal clinical evaluation of the petitioned individual to help make this determination.
When a BHP is made aware of a petition, they should create the person as a client in SmartCare, if not already a client, and enroll them in the CARE Act program. This will allow the CARE Act team to track time spent on that individual and record any related documents, including the petition itself.
The BHP may petition an individual themselves. The SmartCare process does not change much, as the petitioned individual should still be added as a client to SmartCare, if not already, and enrolled in the CARE Act program for tracking.
Information about petitioned individuals, even if they do not ultimately become a CARE participant, is required in the monthly state reporting.
Steps to take when you receive a CARE Act Petition:
- Check to see if the individual is a client. If they aren’t, create them as a client in SmartCare using the Inquiry process.
- Enroll the client in the CARE Act program. You will use this program for all CARE Act related documents and services for this client.
- Scan/upload the petition to the client’s chart in SmartCare. Use “Client (Medical Records)” with Record Type = “CARE Act Petition (scanned)”.
- Create a CARE Episode document to record the petition information.
- Document all activities in the CARE Act program using the appropriate CARE Act Activity procedure codes.
- Complete state reporting requirements.
Active CARE Process and Follow-Up
Once the client is in the CARE Process, meaning attending court, the CARE Act Team will continue to document all activities in the CARE Act program using the appropriate CARE Act Activity procedure codes, as well as completing monthly CARE Act Reporting Documents.
When the client exits the CARE Process, meaning no longer attending court, the CARE Act Team will continue to document all activities in the CARE Act program using the appropriate CARE Act Activity procedure codes, as well as completing monthly CARE Act Reporting Documents.
CARE Act State Reporting
HPs must submit monthly reports to the State on a quarterly basis. The reporting requirements can be found on HMA’s website, https://care-act.org, including the current Data Dictionary, reporting submission file, and submission instructions.
In SmartCare, there are multiple documents and screens that contribute to the state reporting process.
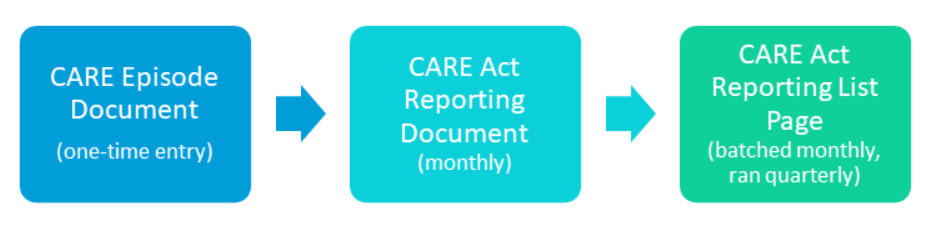
CARE Episode Document: One-time entry
For tracking purposes, CalMHSA has created a concept called the CARE Episode. This is used to track a client’s journey through the CARE Act process. This concept was created so as not to rely on program enrollment data for tracking, which was determined to be inadequate. (See below for decision details.)
For every system referral or petition received, a CARE Episode document should be completed. This is the first step in the state reporting process. Once the CARE Episode document is signed, the system creates the CARE Episode tied to that instigating event. See CARE Episodes for details.
This document should not be edited once signed.
Note on System Referrals that result in a petition: The CARE Episode document records the instigating event that introduced the client to the CARE Act Process. In this situation, the System Referral is that instigating event, not the petition. In this case, DO NOT create a new CARE Episode document for the petition, as it’s simply a follow-up action to the system referral.
Reasons for the CARE Episode Concept
The CARE Process as it’s defined only includes the client’s time within the court process. This includes from petition through graduation. However, the BHP’s requirements go beyond that. They receive referrals for an individual who has not yet been petitioned. They also are required to provide state reporting data for 12 months after a CARE participant has graduated. For counties, that generally means that CARE Act clients are enrolled in the CARE Act program both before and after they are involved with the CARE Act court process.
BHPs also do not have control over other agencies submitting referrals or petitions on a person’s behalf, even if that person is already enrolled in the CARE Act program. DHCS has indicated that all referrals and petitions, even for those clients who are already CARE participants, should be included in monthly state reporting.
CalMHSA built the state reporting documents in SmartCare to minimize duplicative entry by initializing information forward from the previous CARE Act Reporting Document. Without a way to distinguish between the existing ongoing CARE process and a new, duplicate referral, the reporting documents could become inaccurate and messy. Therefore, the CARE Episode concept was created. Now, the system will only initialize information from the previous CARE Act Reporting Document that shares a CARE Episode with the existing document. This should allow staff to document new referrals or petitions on individuals that are already involved with the CARE Act process, without altering the program enrollment.
CARE Act Reporting Document: Monthly
This is where the bulk of the reporting process lives. This document should be completed monthly for each CARE Act client.
As the client moves through the CARE Process, there are different data points that are reported on. The CARE Act Reporting Document is used for all of the CARE Phases, and adjusts the questions based on the phase, as well as the client’s status within that phase.
CARE Phases:
- Referral: Client has been referred using the System Referral process
- Initiation: Client has been petitioned
- Active Service: Client is active in the court CARE Process
- Follow Up: Client is no longer active in the court CARE Process
The CARE Act Reporting Documents should be completed for a client in order. For example, if the client is referred and the referral results in a petition, the CARE Act Team should complete the CARE Act Reporting Document for the Referral phase first, before completing the document for the Initiation phase. This will ensure that the data being pulled into the newest document is the most accurate and has all the necessary information.
Each CARE Act Reporting Document also includes fields for the reporting period. This is limited to one month, per the reporting requirements. However, sometimes a client changes CARE phases during a single month. In this case, a CARE Act Reporting Document must be submitted for each phase included in that month. The reporting period dates allows a user to document when the client moved from one phase to another.
Example: A client is referred via System Referral on 2/2/26. The CARE Act team submits a petition for the client on 2/9/26. The client goes to court and signs a CARE Agreement on 2/24/26.
This client will need 3 CARE Act Reporting Documents for February 2026 with the following phases and respective reporting periods:
- Referral: 2/2/26 – 2/8/26
- Initiation: 2/9/26 – 2/23/26
- Active Service: 2/23/26 – 2/28/26
Active Service Phase
When clients move to the Active Service phase, they will have either a CARE Plan or a CARE Agreement. This is similar to a treatment plan and determines what services the client is recommended to receive. During the CARE Process, the CARE Act Team will be asked to report on whether the client is receiving these services or not. This information is also required for state reporting.
CalMHSA has created the CARE Plan/Agreement document in SmartCare to capture this information. This document simply records what services are on the client’s plan or agreement and whether the form is a CARE Plan or a CARE Agreement. When a client receives a CARE Plan or signs a CARE Agreement, the CARE Act Team should record this in SmartCare using the CARE Plan/Agreement document.
When completing the CARE Act Reporting Document for a client in the Active Service phase, the system will reference the existing CARE Plan/Agreement document and SmartCare’s service information to auto-populate the Services & Supports tab. This tab may take a while to load, as the system is searching for data throughout the system, but should minimize the amount of data entry needed by users.
Sometimes, services haven’t been documented yet, so the CARE Act Reporting Document may not pull in all services that occurred. These fields are editable so that the user can make corrections without having to wait for service entry or the billing process to complete.
Services also don’t match 1:1 from the SmartCare procedure codes to the list of services the CARE Act uses for state reporting. CalMHSA has developed a crosswalk to address this. See CARE Act CPT/HCPCS Code Crosswalk for details.
CARE Act Reporting List Page: Quarterly
Reports are required for each month, and these must be submitted to the State as a separate file for each month. Reports are only due quarterly, meaning three months are often submitted at the same time, although BHPs may submit them more often if desired.
When a BHP is ready to submit a report to the State, they will create a batch submission file, just like any other state reporting item. The CARE Act Reporting List Page is used to create these batches, which can then be extracted, copied into the State’s official submission file template, and submitted via the appropriate State process. See How to Report CARE Act Data for details.
For the CARE Inquiries tab, the BHP should also run the CalMHSA 807 – CARE Act Inquiries Report. This will collect all CARE Act Inquiries for the reporting period for the user to review and add the appropriate summary data to the submission template. See CalMHSA 807 – CARE Act Inquiries Report for details.
Ending the CARE Act Reporting Cycle
The client’s CARE Episode is used throughout the state reporting process. It’s used in the CARE Plan/Agreement document as well as the CARE Act Reporting Document. However, the client eventually leaves the CARE Act process. The CARE Episode is considered closed when the client reaches a stopping status, as reported on the CARE Act Reporting Document, and reporting is no longer required.
CARE Act Related Documents, Screens, and Reports
Documents
- CARE Episode: creates a CARE Episode for the CARE client; should be completed first
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Reporting Document: used to capture monthly reporting data; completed monthly
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Plan/Agreement: used to capture planned services for an active CARE participant; complete as needed during the Active Service period of the CARE Process; update this document before creating the CARE Act Reporting Document that will need to reference this document
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act System Referral: used to create a CARE Act System Referral to be sent to the appropriate BHP
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE System Referral Creation Act-Add On
-
- Read-Only Permission: CARE Act Add-On
- CARE Act Narrative Note: (service note) used to document CARE Act activities for a specific client for most CARE Act activity types
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act 1 Year Status Review Hearing Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Plan Review Hearing Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Case Management Hearing Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Evaluation Review Hearing Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Graduation Hearing Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Hearing on Deferred Ruling Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Initial Hearing Note: (service note) used to document CARE Act activities for a specific client for this specific type of hearing and the hearing on the merits
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Progress/Status Review Hearing Note: (service note) used to document CARE Act activities for a specific client for these specific types of hearing
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Court Document (scanned): used to capture court documents related to CARE Act that are created outside of SmartCare
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act Petition (scanned): used to capture the CARE Act petition created outside of SmartCare
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
- CARE Act System Referral (scanned): used to capture the CARE Act System Referral that was created outside of SmartCare
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, CARE Act-Add On
Screens
- Staff Calendar: uses calendar events to document CARE Act activities not spent on a specific client
-
- No permissions associated with the calendar event types
- CARE Act Services to CPT Codes List: (list page) used to create a crosswalk between SmartCare procedure codes and CARE Act Services and Supports
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin
- CARE Act Services to CPT Codes Details: the detail page associated with the CARE Act Services to CPT Codes List Page
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin
- CARE Act Reporting List Page: (list page) used to create state reporting batches for submissions
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, Billing, Medical Records/Quality Assurance
- CARE Act Record Details: the detail page associated with the CARE Act Reporting List Page
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, Billing, Medical Records/Quality Assurance
Reports
- CalMHSA 807 – CARE Act Inquiries Report: used for state reporting CARE Act inquiries
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, Medical Records/Quality Assurance
- CalMHSA 207 – CARE Act Claim Report: used for CARE Act activity reimbursement
-
- Read/Write Permissions: CalMHSA Sys Admin, County Affiliate Sys Admin, Billing, Medical Records/Quality Assurance
User Roles
CARE Act Add-On: Give to users on the CARE Act Team. This provides them permissions to view and create CARE Act related documents.
CARE Act System Referral Creation Add-On: Give to users who are able to create a CARE Act System Referral. Only people with certain license types working within certain types of programs are allowed to create a CARE Act System Referral.