Mental Health Rehabilitation Centers (MHRCs) are one of the few types of programs that require a client plan that is signed by the client and guardian. It is for this reason that CalMHSA recommends using the Interdisciplinary Treatment Plan for this requirement.
How to Create an Individual Service Plan
- Navigate to the Interdisciplinary Treatment Plan
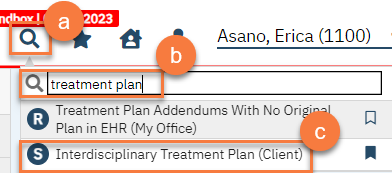
- With the client open, click on the Search icon.
- Type in “Interdisciplinary Treatment Plan” in the search bar.
- Click to select “Interdisciplinary Treatment Plan (Client)” from the search results.
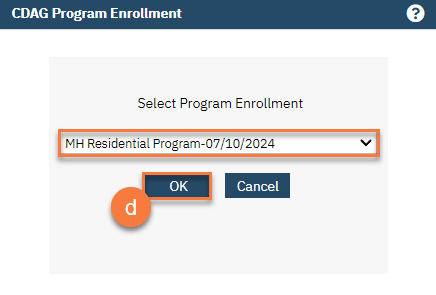
- If this is the first Interdisciplinary Treatment Plan for the client, you’ll receive a CDAG Program Enrollment pop-up window. Select your program from the dropdown and click OK.
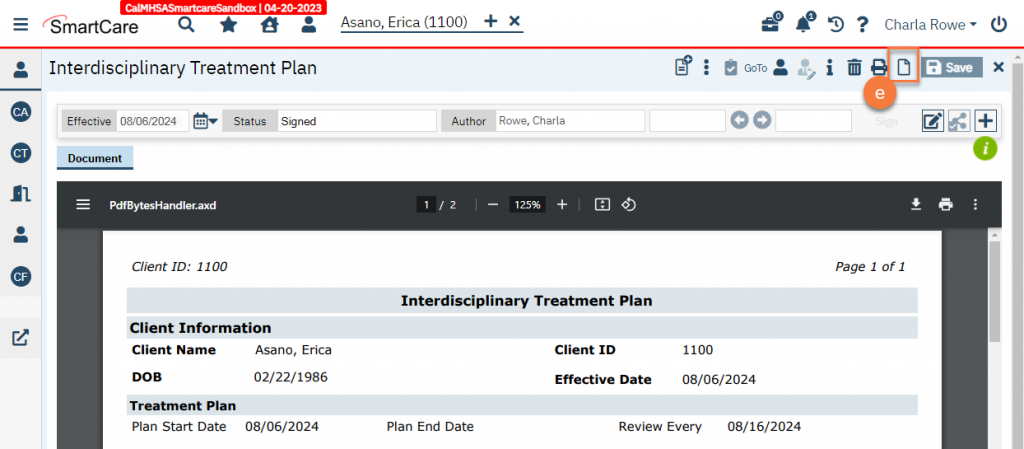
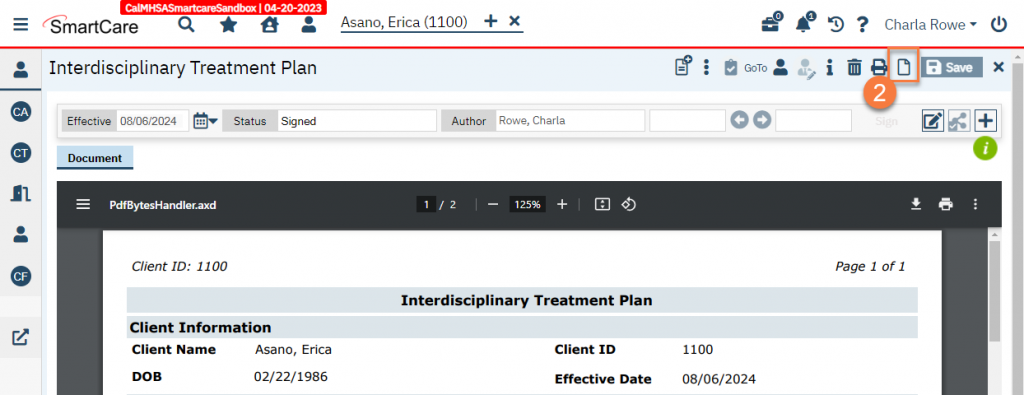
- If this is not the first Interdisciplinary Treatment Plan for the client, you’ll see the most recent plan in PDF view. Click on the New icon to create a new Interdisciplinary Treatment Plan.
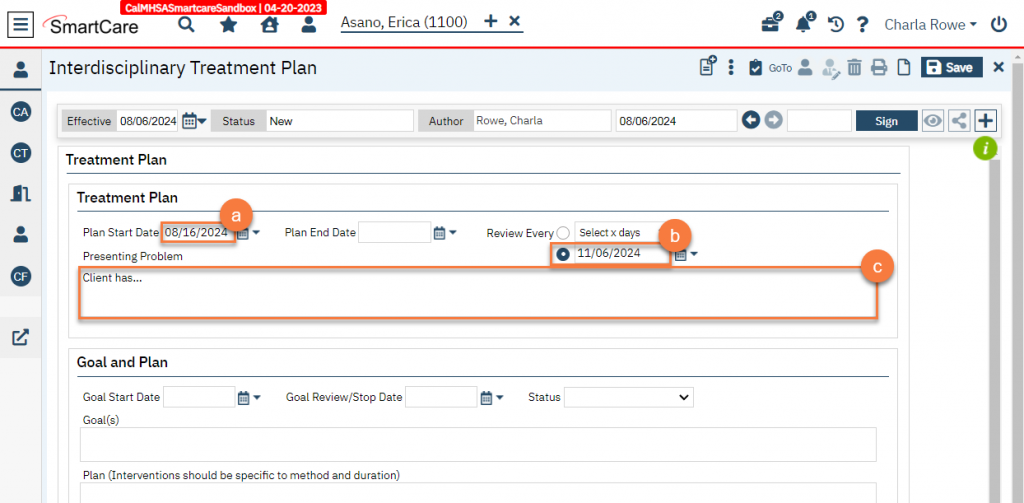
- Complete the Treatment Plan section.
- Enter the state date of the new treatment plan. Leave the end date blank if the plan is still active.
- In the “Review Every” field, select the radio button next to the date field. Enter when the next review is due by entering the date 3 months from the start date. This indicates the due date of the quarterly review.
- Enter the presenting problems. This should include the specific treatment/rehabilitation needs of the client.
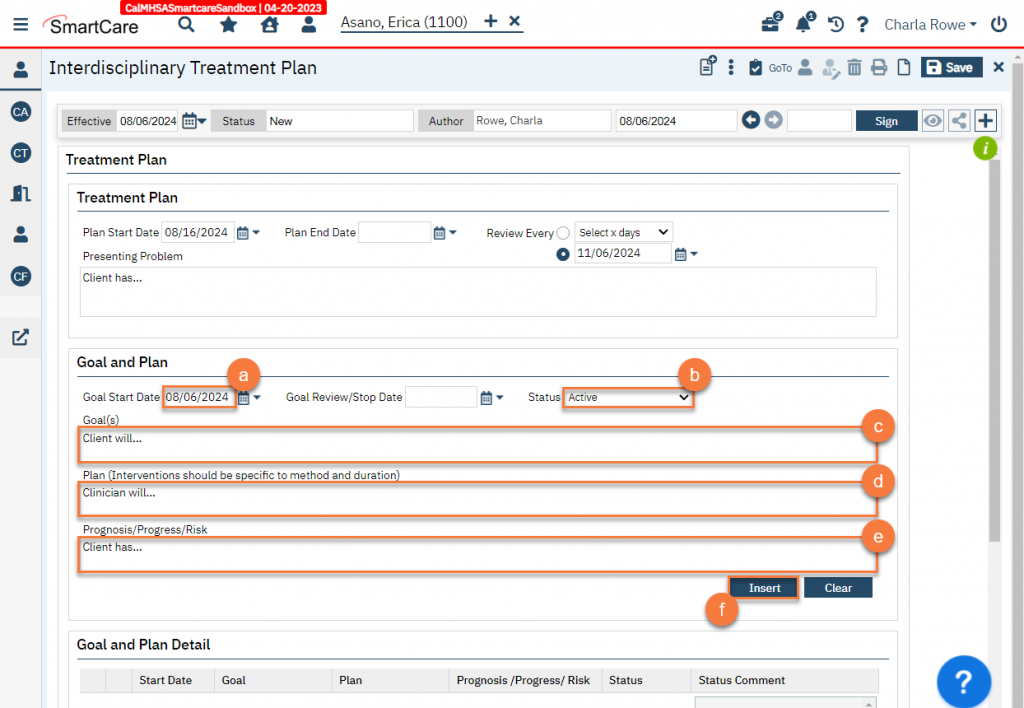
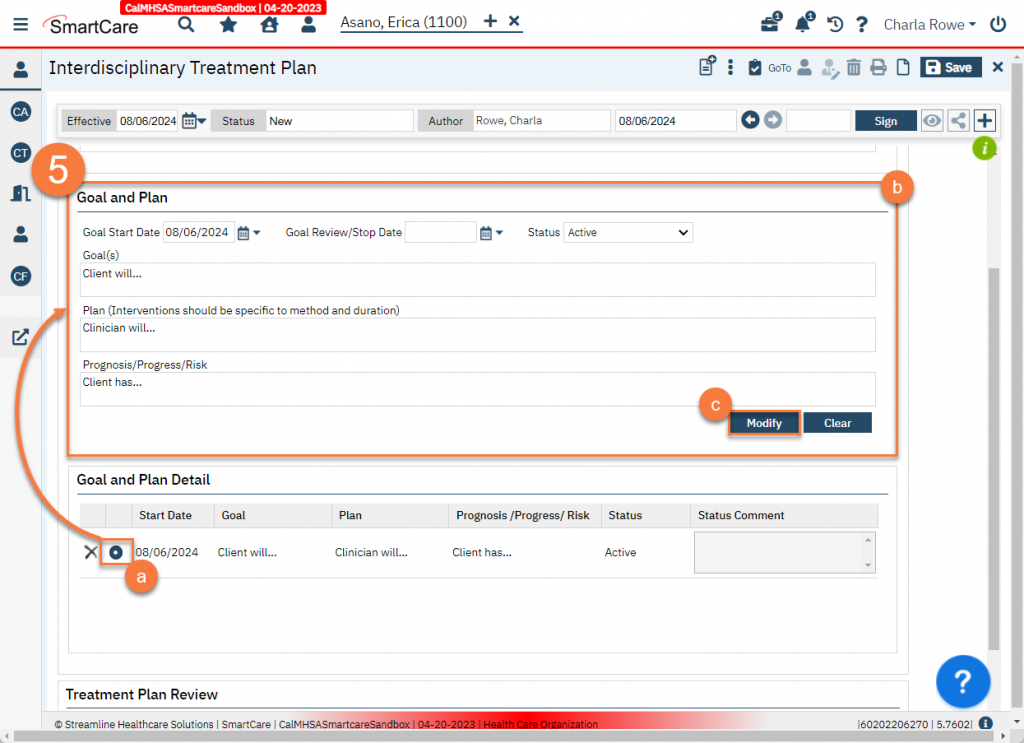
- Enter goals and plans – each goal will have a plan and prognosis associated with it.
- Enter the start date of this goal. This should be when the goal was identified as ready to be worked on. Leave the Goal Review/Stop Date blank as this is an active goal.
- Enter the status of the goal as “Active”. “Active” means the goal is currently being worked on. “Completed” means the client has successfully met the goal. “Discontinued” means the client has not successfully met the goal but the goal is no longer being actively worked on.
- Enter the first goal. Goals should be specific and include measurable objectives.
- Enter the plan to address that goal. This includes the responsibilities of both the staff and the client to achieve the goal, the services to be provided, and the staff responsible for the provision of each service.
- Enter the prognosis and any risk factors associated with the completion of this goal.
- Click Insert.
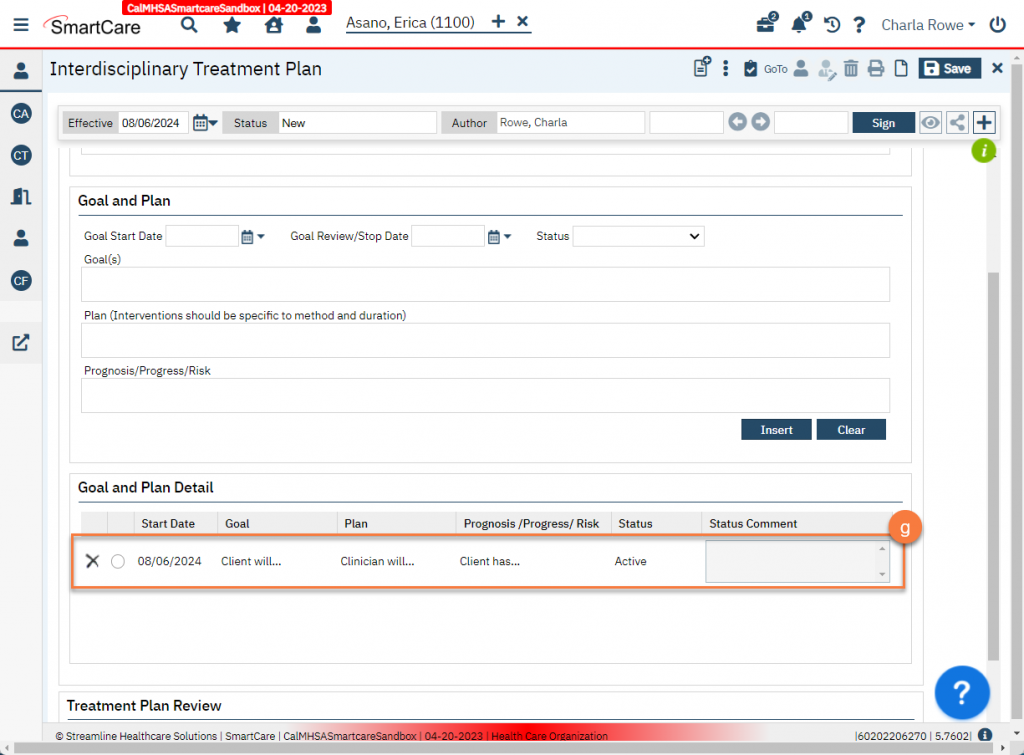
- This will add the goal to the “Goal and Plan Detail” section. Repeat a-f until all goals have been entered.
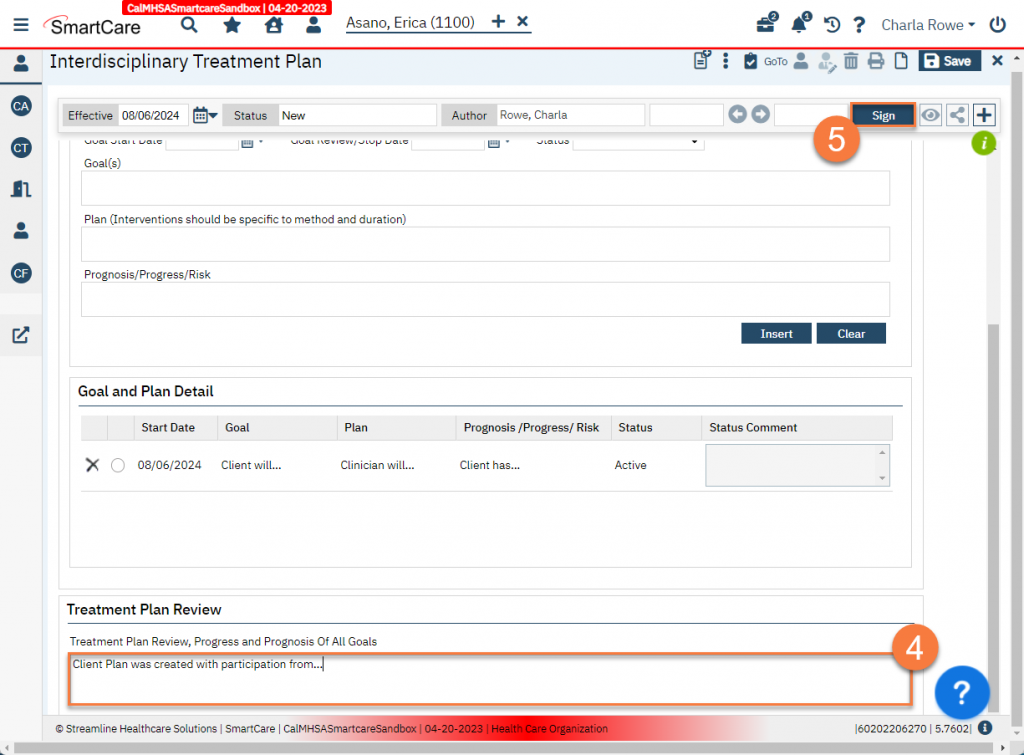
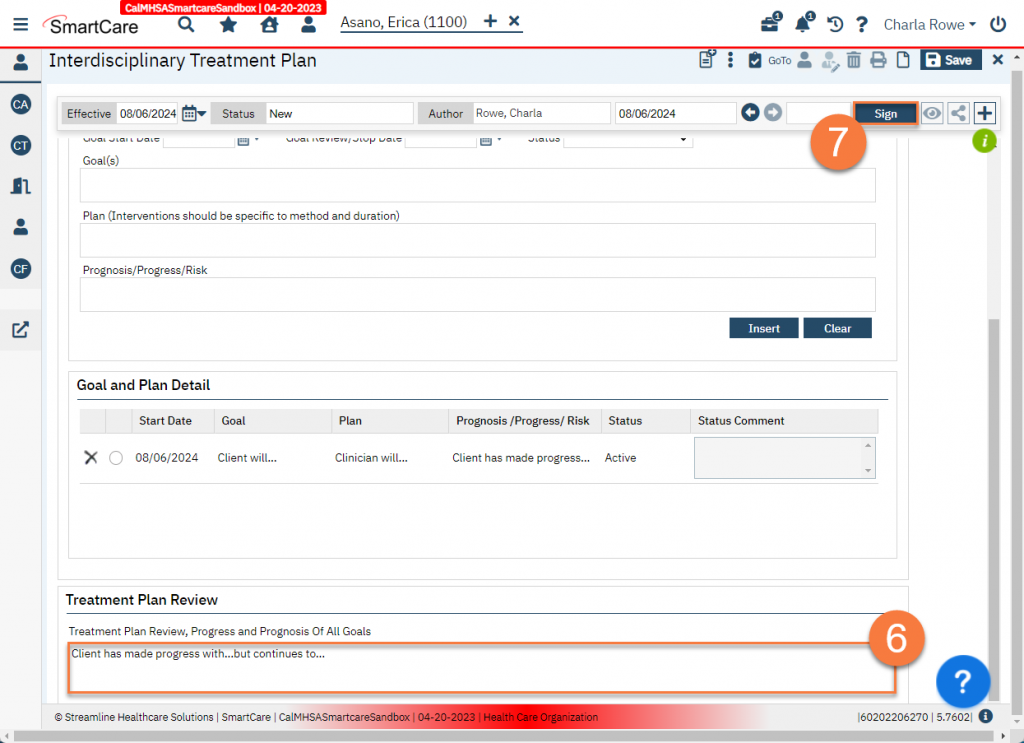
- Enter a summary of the treatment plan in the Treatment Plan Review field.
- Click Sign to complete the document.
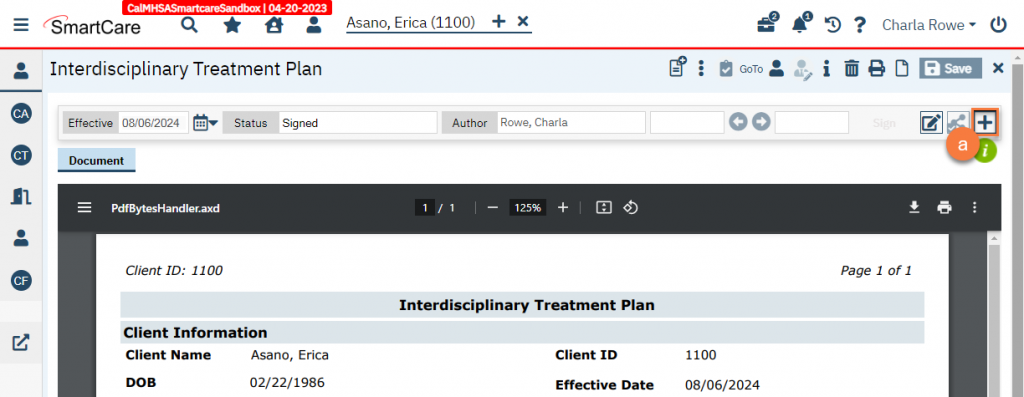
- Add co-signers as necessary.
- Click the plus button on the document ribbon to expand it.
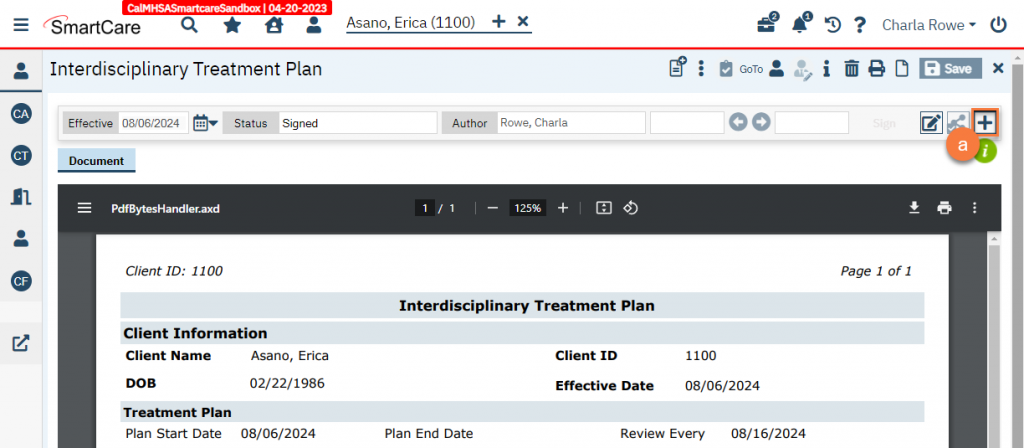
- Ensure the client and guardian are included. These should be included automatically as co-signers.
- To add more co-signers, click in the “Add Signer(s)” field. This will bring up a dropdown. If you do not see the person you’re expecting to, click on Other Signer(s).
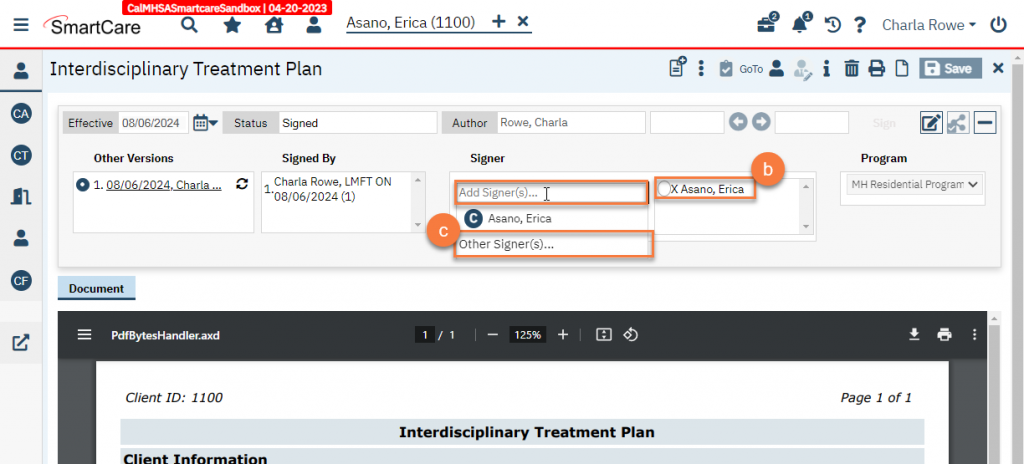
- This will bring up a popup window. Enter in the person’s name and their relationship to the client. Click OK.
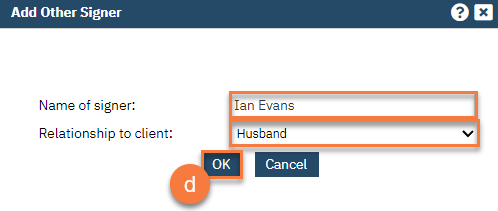
- This will add the person to the co-signer list.
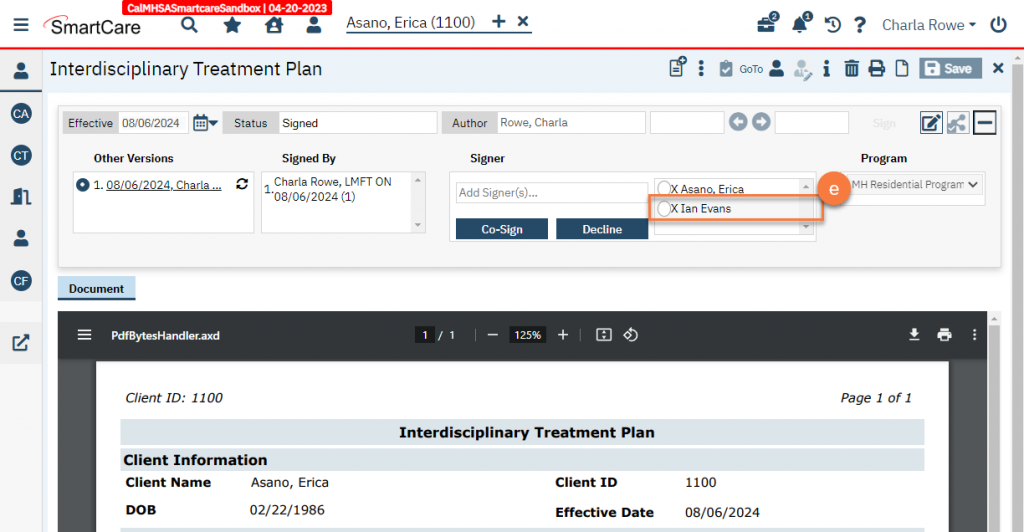
- Gain the client’s signature. If the client is unable or unwilling to sign, document this by selecting the client from the co-signer list and click Decline.
- Gain the guardian’s signature, and the signature of any other co-signers.
- Write a service note documenting the creation of the treatment plan. This service note should document who participated in the creation of the treatment plan.
Monthly Reviews
The treatment plan needs to be reviewed by staff and clients on at least a monthly basis. Formal review and updates must be done on a quarterly basis. Monthly reviews that do not require updates can be documented in services notes. Make sure to include the client’s involvement in the review, as well as the expected length of stay for the client in order to accomplish the identified goals, and the methods of evaluating the achievement of these goals.
Quarterly Reviews
Every quarter, the individual service plan should be reviewed and updated. This update can occur more frequently as clinically appropriate. To update the service plan, follow the steps below.
- Navigate to the Interdisciplinary Treatment Plan
- With the client open, click on the Search icon.
- Type in “Interdisciplinary Treatment Plan” in the search bar.
- Click to select “Interdisciplinary Treatment Plan (Client)” from the search results.
- Click on the New icon.
- This will bring up the CDAG Program Enrollment popup. Select your program and click OK.
- This will pull forward some information from the previous treatment plan. Enter in the new information for this updated treatment plan.
- Enter the state date of the new treatment plan. Leave the end date blank if the plan is still active.
- Enter when the next review is due by entering the date 3 months from the start date.
- Update the presenting problems section as necessary.
- Make updates as necessary to goals and related plans.
- Click on a goal in the “Goal and Plan Detail” section to select it and bring the information into the “Goal and Plan” section.
- Update the fields in the Goal and Plan section as necessary. In the “Prognosis/Progress/Risk” field, include any progress made on this goal.
- To end a goal, enter the Goal Review/Stop Date and change the Status to either “Discontinued” or “Complete”.
- Click Modify to save these changes.
- Repeat steps a-c until all goals are updated.
- Enter a summary of the review and update in the Treatment Plan Review field. Include a summary of the client’s progress, the appropriateness of identified needs, client goals and objectives, and the success of the plan.
- Click Sign to complete the document.
- Add co-signers as necessary.
- Click the plus button on the document ribbon to expand it.
- Ensure the client and guardian are included. These should be included automatically as co-signers.
- To add more co-signers, click in the “Add Signer(s)” field. This will bring up a dropdown. If you do not see the person you’re expecting to, click on Other Signer(s).
- This will bring up a popup window. Enter in the person’s name and their relationship to the client. Click OK.
- This will add the person to the co-signer list.
- Gain the client’s signature. If the client is unable or unwilling to sign, document this by selecting the client from the co-signer list and click Decline.
- Gain the guardian’s signature, and the signature of any other co-signers.
- Write a service note documenting the review and update of the treatment plan. This service note should document who participated in the review, including the client and any relevant collateral contacts.
- The written individual service plan shall be prepared within 30 days following admission by the program director or a staff member that is a licensed mental health professional, and shall include, but not be limited to, the following:
- Specific goals and measurable objectives, the staff and client’s responsibilities for their achievement.
- Statement of specific treatment/rehabilitation needs and goals.
- The individual service plan shall indicate the services to be provided, the objectives to be accomplished, and the staff responsible for the provision of each service.
- The objectives shall be measurable, with time frames, and shall be reviewed and updated at least monthly.
- Specific goals and measurable objectives, the staff and client’s responsibilities for their achievement.
- There shall be weekly progress notes in the record for each client which shall include notes written by members of the program staff or interdisciplinary professional staff providing rehabilitation services to the client. The notes shall be a general review of weekly progress.
- Documentation of reviews by staff and clients of the individual service plan on at least a monthly basis.
- Clients shall be involved in an on-going review of progress towards goal attainment and in the planning and evaluation of their treatment/rehabilitation goals.
- Anticipated length of stay for the client in the mental health rehabilitation center needed to accomplish identified goals,2and methods to evaluate the achievement of these goals.
- There shall be a review and updating of the individual service plan as necessary but at least quarterly, and more often if there is a change in the client’s condition.
- The quarterly review shall include a reevaluation which shall be a summary of the progress of the client in the rehabilitation program, the appropriateness of identified needs, client goals and objectives and the success of the plan.
- The client should be present at the quarterly review and if agreed to by the client, family members may be notified and attend the quarterly review.
- The service plan shall be approved by the program director or a licensed mental health professional, and signed by the client.
- Prior to discharge, there shall be a written discharge summary prepared by the staff which shall include an outline of services provided, goals accomplished, reason and plan for discharge, and referral follow-up plans.
- At least every four (4) months, the mental health rehabilitation center in conjunction with the local mental health director or designee, shall reassess each client to determine the need for continued placement of the client in the mental health rehabilitation center.
Updated 8/6/24